Educational Theory
Because understanding how people learn will make you a better teacher — and, quietly, a much better learner too.
path: EDUCATIONAL THEORIES
- 2 minutes on educational change.doc
- 2 minutes on motivation for learning.docx
- 2 minutes on the development cycle.doc
- a beginners guide to teaching (with slide notes).ppt
- abc of learning and teaching - BMJ links.doc
- adult learners vs children.ppt
- blooms taxonomy and task design (TEACHING RESOURCE).doc
- blooms taxonomy chart for learner reflection.doc
- blooms taxonomy.doc
- competence - 4 levels of competence.doc
- competency - the four levels.doc
- creating teaching materials.pdf
- curriculum ignorance map.doc
- desktop.ini
- dialogue or discussion.doc
- dialogue versus discussion (TEACHING RESOURCE).pdf
- educational cycle.doc
- educational paradigm.doc
- educational theory in practice.pdf
- elearning - usability testing.doc
- emotional intelligence.pdf
- group cohesion.ppt
- group facilitation - tuckman.doc
- how can we teach effectively.ppt
- how we learn.ppt
- johari window model.pdf
- kolbs cycle.pdf
- kolbs learning cycle.ppt
- learning strategies.ppt
- life long learning bmj.pdf
- maslow and self-actualisation.docx
- maslow and short index self actualisation questionnairre.doc
- maslow self actualising needs analysis.pdf
- maslows heirarchy in practice.doc
- maslows heirarchy of needs one side of A4.doc
- methodology - 6 principles - good and mccaslin.doc
- millers pyramid - assessing competence and performance.pdf
- motivation for learning - 2 minute guide.rtf
- PUNs and DENs to RUNs and TENs.ppt
- questionnaires - designing.doc
- rosenshines 17 principles of effective teaching.pdf
- rosenshines principles of effective instruction.pdf
- RUNS and TENs grid - example.doc
- social cognitive theory - an overview on Badura.docx
- social cognitive theory - key constructs.doc
- social cognitive theory - reciprocal determinism.docx
- social cognitive theory essay.pdf
- socratic dialogue.doc
- socratic questioning.doc
- top ten educational pearls.doc
- vellas 12 principles for effective adult learning.pdf
A hand-picked mix of official guidance and real-world GP training resources. Because sometimes the best pearls are not hiding in the official documents.
Knowles — Andragogy
Adults need to know why they are learning. They bring experience. They want relevance, autonomy, and problem-solving — not lectures.
Pedagogy vs Andragogy
Not a battle — a spectrum. Use pedagogic (teacher-led) methods for rapid updates; use andragogic (learner-led) methods for lasting change.
Constructivism
Learners build understanding by connecting new knowledge to what they already know. No two people learn exactly the same thing.
Gibbs' Reflective Cycle
6 steps: Description → Feelings → Evaluation → Analysis → Conclusion → Action Plan. Perfect for case-based learning and ePortfolio entries.
Kolb's Learning Cycle
Experience → Reflect → Conceptualise → Experiment. Learning is active, not passive. Reflection alone is not enough — you must act.
Maslow's Hierarchy
A trainee who is exhausted, unsafe, or unhappy cannot learn effectively. Always check the basics before expecting high-level engagement.
Bloom's Taxonomy
6 levels: Remember → Understand → Apply → Analyse → Evaluate → Create. Good teaching targets higher levels. AKT tests all six.
Miller's Pyramid
Knows → Knows How → Shows How → Does. AKT = bottom two levels. SCA = upper two levels. Aim for the apex in real practice.
Grow's Model
Match your teaching style to the trainee's current level of self-direction. Dependent learners need guidance; self-directed learners need space.
Tuckman's Stages
Forming → Storming → Norming → Performing (→ Adjourning). Groups must be allowed to storm. Skipping this stage creates dysfunction later.
Educational theory is not something invented by academics to make your life more complicated. It is a set of well-tested ideas about how people actually learn — and once you understand them, you will notice them everywhere: in every tutorial, every teaching session, every exam, and every consultation.
Knowles' Principles of Adult Learning — Andragogy
Knowles asked a deceptively simple question: do adults learn differently from children? His answer was yes — and the word he coined for adult-centred teaching is Andragogy (from the Greek for "man-leading"), as opposed to Pedagogy ("child-leading").
Teacher-led
Learner passive
Learner-led
Teacher facilitates
| Principle | What it means | In practice for GP training |
|---|---|---|
| 1. Need to Know | Adults want to understand why before investing effort | Start every tutorial: "Here's why this matters for your real clinics…" |
| 2. Self-Concept | Adults see themselves as capable, self-directed learners | Avoid being patronising. Involve them in choosing what to cover |
| 3. Prior Experience | Adults bring a rich bank of life and work experience | Build on what they already know. Ask what they've seen in clinics |
| 4. Readiness to Learn | Adults learn best when the topic is immediately relevant | Use recent cases. Connect content to what's happening in their post |
| 5. Problem Orientation | Adults prefer learning around problems, not abstract theory | Case-based discussion, PUNs & DENs, scenario-based tutorials |
| 6. Intrinsic Motivation | Internal drives (growth, competence) matter more than external rewards | Praise professional development, not just exam performance |
Insider Tip — What Trainees Actually Say
The most common complaint from GP trainees about tutorials: "It didn't feel relevant to what I'm actually doing." That is a direct failure to apply Principle 4 (Readiness to Learn). The fix is almost always the same: start with a real case from the trainee's own week, then work backwards into the theory.
Constructivism — The 3 Cs
Constructivism says that people learn best by actively building their own understanding — fitting new information into what they already know. You cannot simply transfer knowledge into someone else's head. The learner has to construct meaning themselves.
Gibbs' Reflective Cycle
Gibbs' cycle gives you a structured framework for reflection — particularly useful for emotionally charged clinical experiences. It ensures that reflection does not stay as vague feelings but translates into real learning and changed behaviour. It is also the backbone of good ePortfolio entries on FourteenFish.
| Where | How | Key tip |
|---|---|---|
| Tutorial discussions | Use the six headings to structure any case or critical incident discussion | Do not rush past Stage 2 (Feelings) — emotional processing is where real learning starts |
| FourteenFish ePortfolio | Teach trainees to structure their Learning Log entries using Gibbs | Entries that reach Stage 6 (Action Plan) demonstrate genuine reflection — those that stop at Stage 1 do not |
| Personal development | Encourage trainees to apply Gibbs to a challenging consultation privately | The goal is not self-criticism — it is self-understanding. Evaluation must include what went well |
Kolb's Experiential Learning Cycle
Kolb's cycle describes how people learn through doing and reflecting. It has four stages, and — crucially — you can enter the cycle at any point. The cycle only works if all four stages are completed.
Maslow's Hierarchy of Needs
Maslow proposed that each of us is motivated by a hierarchy of needs — and that lower needs must be reasonably satisfied before we can engage with higher ones. In an educational context, this explains why some trainees seem unable to engage in learning, no matter how good the teaching is.
- When a trainee seems unmotivated, think Maslow first
- Check: are basic needs being met? Sleep, safety, wellbeing?
- Esteem needs: does the trainee feel respected and valued?
- Belonging: do they feel part of the team?
- Only when lower needs are met can they reach self-actualisation — genuine learning
- Marital difficulties (belonging) do not automatically destroy esteem
- Helping others (higher level) can actually lift someone from lower-level difficulty
- Humans move up and down the hierarchy throughout their lives
- Use it as a lens, not a diagnosis
Bloom's Taxonomy of Learning
Bloom's taxonomy describes six levels of learning — from basic recall of facts right up to the ability to create something new. Understanding these levels will completely change how you design teaching objectives, write exam questions, and set learning goals for trainees.
| Level | What it means | Example action verbs | In GP training |
|---|---|---|---|
| 1. Remember | Recall facts and basic concepts | List, name, recall, define | Name the diagnostic criteria for depression |
| 2. Understand | Explain ideas or concepts | Summarise, explain, describe | Explain how antidepressants work |
| 3. Apply | Use knowledge in new situations | Use, solve, demonstrate | Choose the right antidepressant for this patient |
| 4. Analyse | Draw connections; break down information | Differentiate, examine, compare | Compare SSRIs vs SNRIs for this clinical context |
| 5. Evaluate | Justify a decision or position | Defend, argue, judge, critique | Evaluate whether this prescription was appropriate |
| 6. Create | Produce new work or ideas | Design, construct, develop | Design a QI project to improve depression care |
Miller's Pyramid of Clinical Competence
Miller's pyramid describes four levels of clinical competence — from knowing facts right up to doing the right thing naturally in real practice. It is widely used in medical education to design assessments and understand the gap between "knowing" and "doing."
| Level | Description | How assessed in MRCGP |
|---|---|---|
| Knows | Can recall factual knowledge | AKT — written MCQ exam |
| Knows How | Can apply knowledge to clinical scenarios | AKT extended matching and data interpretation |
| Shows How | Can demonstrate competence in a controlled setting | SCA — simulated consultation |
| Does | Performs competently in real unsupervised practice | WPBA — COT, CbD, MSF, observed in real clinics |
Grow's Model for Staged Self-Directed Learning
Grow translated leadership theory from the business world into education. His core idea is simple: your teaching style must match the learner's current level of self-direction. Use the wrong style — even if it is brilliant teaching — and you will either overwhelm or bore them.
| Stage | Learner | Teacher | Methods that work | Pitfall to avoid |
|---|---|---|---|---|
| Stage 1 | Dependent — needs direction, low confidence or new to topic | The Expert — authoritative, directive | Direct instruction, coached feedback, clear explanation, demonstrations | Being so controlling that you stifle initiative and create permanent dependency |
| Stage 2 | Interested — motivated but still needs structure | Motivator — inspiring but providing frameworks | Inspiring lecture + guided discussion, goal-setting, learning strategies | Entertaining well but leaving the trainee with no practical learning skills |
| Stage 3 | Involved — engaged and increasingly self-directing | Facilitator — equal partner in discussion | Facilitated group discussion, collaborative small group work, problem-based learning | Accepting and validating everything — trainees then show little respect or challenge |
| Stage 4 | Self-directed — autonomous, takes initiative for own learning | Delegator — mentor who monitors from a distance | Internship-style learning, self-directed projects, mentorship, audit, research | Withdrawing so far that you lose touch and fail to monitor progress |
- Stage 1 learner + Stage 4 teacher: The trainee feels abandoned and lost. They needed guidance and got space they weren't ready for.
- Stage 4 learner + Stage 1 teacher: The trainee feels patronised and micromanaged. They had the ability and were not trusted to use it.
Tuckman's Stages of Group Development
Tuckman described how groups develop over time. Understanding this model is essential for anyone facilitating VTS half-day release sessions, small group tutorials, or any new team. Groups that do not go through all four stages rarely perform well — and the storming stage is not something to eliminate; it is something to manage.
Forming
Polite. Cautious. Everyone on best behaviour. Group members are still figuring out who everyone is.
Storming
Conflict and tension emerge. Opinions clash. Leadership is challenged. Uncomfortable — but vital.
Norming
Group settles. Rules and roles become clear. Trust starts to build. Conflict resolves.
Performing
The group is functional, collaborative, and productive. This is the goal.
- Allow enough time for Forming — introductions, ice-breakers, establishing norms
- When Storming begins: do not shut it down. Facilitate it safely
- Familiar groups move through early stages faster — adjust accordingly
- Tuckman applies equally to MDT teams, not just educational groups
The Johari Window is a model for understanding self-awareness — relevant to both clinical development and educational relationships. It divides self-knowledge into four quadrants:
This model describes the four stages of skill acquisition — widely used in clinical training to understand how expertise develops.
| Level | Description | Example in GP |
|---|---|---|
| 1. Unconscious Incompetence | You do not know what you do not know — blissful ignorance | A new ST1 who does not realise how complex a consultation is |
| 2. Conscious Incompetence | You now know what you cannot do — the uncomfortable awareness stage | A trainee who realises mid-clinic that they are struggling with ICE |
| 3. Conscious Competence | You can do it — but it requires deliberate effort and concentration | A trainee who remembers to explore ICE if they consciously try |
| 4. Unconscious Competence | You do it naturally without thinking — true expertise | An experienced GP who explores ICE automatically without thinking about it |
Cognitive Load Theory, developed by John Sweller, describes the limits of working memory. The brain can only hold a limited amount of new information at once — and overloading it is one of the most common teaching mistakes.
- Do not cram 40 slides into a 45-minute session. Less content, done well, is more effective
- Use clear, simple visuals — cognitive overload kills learning faster than anything
- Chunking information into small pieces reduces intrinsic load
- Worked examples are more effective than problem-solving at early stages of learning
- Revision spacing over time moves learning from working memory into long-term memory
Albert Bandura demonstrated that much of human learning happens through observing others — not just through direct experience. He also introduced the concept of self-efficacy: your belief in your own ability to succeed in a specific situation.
PUNs and DENs is a practical educational tool that bridges Knowles' principle of problem-orientation with Kolb's experiential learning cycle. It turns clinical uncertainty into structured learning needs.
| Theory | Author | Core idea in one line | Most useful for |
|---|---|---|---|
| Andragogy | Knowles, 1984 | Adults learn best when they know why, bring experience, and choose relevance | Tutorial design, PDP conversations, understanding trainee motivation |
| Constructivism | Vygotsky/Piaget | Learners construct their own understanding — they are not empty vessels | Small group facilitation, problem-based learning, case discussions |
| Gibbs' Cycle | Gibbs, 1988 | Structured reflection through six stages from description to action plan | Case-based reflection, ePortfolio writing, post-incident learning |
| Kolb's Cycle | Kolb, 1984 | Learn through doing, reflecting, conceptualising, and experimenting — all four stages | Understanding the full learning cycle; linking experience to theory |
| Maslow's Hierarchy | Maslow, 1943 | Lower needs must be met before higher-level learning engagement is possible | Understanding demotivated trainees; trainee wellbeing discussions |
| Bloom's Taxonomy | Bloom 1956/revised 2001 | Six levels from recall to creation — good teaching targets the upper levels | Writing learning objectives, designing questions, AKT preparation |
| Miller's Pyramid | Miller, 1990 | Knows → Knows How → Shows How → Does — the hierarchy of clinical competence | Understanding MRCGP assessments; designing work-based learning |
| Grow's Model | Grow, 1991 | Match teaching style to the learner's current level of self-direction | Tutorial planning, identifying why teaching is not landing |
| Tuckman | Tuckman, 1965 | Groups go through Forming → Storming → Norming → Performing | VTS facilitation, MDT teamwork, understanding group difficulties |
| Johari Window | Luft & Ingham | Self-awareness has four quadrants — feedback and openness expand the "Open Area" | Feedback conversations, MSF discussions, personal development |
| 4 Levels of Competence | — | Unconscious incompetence → Conscious incompetence → Conscious competence → Unconscious competence | Normalising the difficulty of Stage 2 for trainees who feel overwhelmed |
| Cognitive Load Theory | Sweller | Working memory is limited — reduce extraneous load, support germane load | Designing teaching sessions; why less content done well is more effective |
| Social Cognitive Theory | Bandura | We learn through observation; self-efficacy shapes what we believe we can achieve | Role modelling, positive feedback, building trainee confidence |
Reflection & the FourteenFish ePortfolio — What Trainees Actually Find Hard
Reflection is the single most misunderstood part of GP training. Virtually every trainee struggles with it at first — and most of the struggle comes from the same few mistakes, repeated over and over. Here is what trainees consistently report finding difficult, and what actually helps.
Most trainees write too much description and too little analysis. Flip it: keep the description brief and invest your effort in the lower two sections.
| ❌ What trainees do | ✅ What supervisors want instead |
|---|---|
| Write a long, detailed account of exactly what happened — a clinical story | Brief description only — just enough context so the reader knows what you are reflecting on. Then move straight to analysis |
| Leave out feelings entirely — "I managed the patient and discharged them" | Name the emotion, even briefly: "I felt uncertain when…" or "I was worried because…" — this is what makes it personal and reflective |
| Say what they would do the same without explaining why | Justify every decision — "I would do X again because Y, and next time I would also consider Z" |
| Write entries in batches just before the ESR review | Write steadily throughout — one or two a week. Supervisors can see the dates. Batching also means you get all the feedback at once, which you cannot act on before the next entry |
| Reflect on the same types of case repeatedly | Check your capability coverage regularly in FourteenFish. Target gaps deliberately — especially Community Orientation, which is often the hardest to evidence in hospital posts |
| Criticise colleagues: "My registrar did X wrong and I had to fix it" | Focus only on your own learning. Entries criticising others reflect poorly on you and cannot be used to demonstrate your own competence |
| Set vague learning needs: "I want to learn more about diabetes" | Be SMART: "By the end of this rotation, I will attend one diabetic clinic and write a reflection linking to the Long-Term Conditions clinical experience group" |
| Aim for perfect entries from day one | Start writing, even imperfectly. No supervisor expects brilliance in week one. They expect to see improvement over time — that IS the evidence of development |
Research shows that up to 80% of international medical graduates have never encountered reflective writing before coming to the UK. This is entirely normal — reflective practice simply is not part of many countries' medical training. It is a skill, not a talent. Here is what IMGs consistently report helping:
- Start with a verbal reflection — before writing, talk through the case with your trainer using Gibbs' headings. Most people find it easier to speak first, write second
- Focus on the reaction, not the facts — the medico-legal concerns about detailed factual records are real. Reflection that focuses on your response to an event is safer and also more educationally valuable than a clinical summary
- Short is fine — one strong paragraph of genuine analysis is more valuable than three paragraphs of description. Quality, not length, is what supervisors are looking for
- Link to the 13 capabilities from the start — this gives structure when you are not sure what to write about. Ask: "Which capability did this test? How did I demonstrate it — or where did I fall short?"
Honey & Mumford — Knowing Your Learning Style Changes Everything
Honey and Mumford took Kolb's four-stage cycle and turned it into something trainees can actually use on themselves. They gave each stage a name — a "learning style" — that describes the kind of learner who naturally gravitates to that stage. Knowing your style does not box you in. It shows you where you are already strong — and where you need to push yourself.
| Honey & Mumford Style | Kolb Stage they prefer | Their natural strength | What to stretch towards |
|---|---|---|---|
| Activist | Concrete Experience (Stage 1) | Getting stuck in, trying new things | Reflective Observation — slow down and think it through |
| Reflector | Reflective Observation (Stage 2) | Thoughtful analysis, thorough reflection | Active Experimentation — act on the conclusions |
| Theorist | Abstract Conceptualisation (Stage 3) | Understanding evidence, building frameworks | Concrete Experience — get comfortable with ambiguity in real practice |
| Pragmatist | Active Experimentation (Stage 4) | Applying knowledge to real problems | Reflective Observation — pause to ask "why did that work?" |
Insider Tip — From UK Trainers
Your Educational Supervisor may ask you to complete the Honey & Mumford Learning Styles Questionnaire early in your GP attachment. Many trainees dismiss it as a tick-box exercise. The trainers who get the most out of it use it as a genuine conversation-starter: "I'm a Reflector — so why do I keep avoiding writing up my learning needs?" Understanding your style is the first step to working with it, not against it.
What Trainees Consistently Get Wrong — About Learning and Educational Theory
These are the recurring mistakes that GP trainers and educational supervisors see again and again, year after year — on reflective entries, in tutorials, and in conversations about learning. None of them are catastrophic. All of them are easy to fix once you know what to look for.
This is the most common mistake of all. Description is not reflection. You can write two pages about exactly what happened in a consultation and your educational supervisor still cannot award a single professional capability — because you have described, not reflected.
The FourteenFish ePortfolio is consistently described by trainees as "time-consuming" and "stressful." That is understandable — especially in busy rotations. But the trainees who change their relationship with it from "something I have to do" to "something that helps me" are the ones who get the most out of training.
Many trainees report waiting weeks before writing entries because "nothing interesting has happened." This is a mistake on two levels. First, interesting things happen every single day in general practice — they just do not feel interesting until you stop and reflect on them. Second, the most educationally valuable cases are often the ones that felt ordinary at the time but reveal something deeper on reflection.
One of the biggest sources of anxiety in early training is receiving NFD grades on the FourteenFish ePortfolio. Trainees coming from medical school or foundation training are used to being graded "Excellent" — and seeing NFD looks alarming. But it should not be.
Many trainees — especially those preparing to become trainers — can name Bloom's levels, recite Gibbs' stages, and explain Tuckman's model fluently. But they then run tutorials that are entirely teacher-led, with no reflection component, no connection to the trainee's own experience, and no follow-up action. That is pedagogy masquerading as andragogy.
What the Best GP Learners Actually Do — Evidence and Insider Wisdom
There is a clear pattern among trainees who progress smoothly through training, pass their exams with confidence, and feel genuinely well-prepared for independent practice. They are not always the most naturally gifted clinicians. They are the ones who have turned educational theory into personal habit.
There is growing awareness in UK GP training of trainees using AI tools to generate portfolio entries. The temptation is understandable — reflection is hard, time is short. But this misses the point entirely.
The value of reflection is not the written product — it is the process of thinking. A beautifully written AI-generated reflection that bypasses genuine thought produces no learning whatsoever, and is effectively plagiarism in the context of a professional training programme.
The constructive use of AI for reflection is different: using it to prompt you with questions ("What did I feel in that moment? What would I do differently?"), to structure your thoughts, or to check your action plan is realistic — not to write the reflection for you. The thinking must remain yours. This aligns with BJGP guidance and GMC confidentiality requirements.
Transformative Learning — The Hidden Goal of GP Training
Mezirow proposed that the most powerful form of adult learning goes beyond adding new knowledge — it changes the way you think. He called this transformative learning: a fundamental shift in how you see yourself, your role, and the world around you.
This is precisely the philosophy behind Bradford VTS: not just imparting knowledge, but creating fundamental changes in thoughts, feelings, attitudes, and behaviour. Not making you cleverer — making you a different and better kind of doctor.
| Blind Spot | What it looks like | How to address it |
|---|---|---|
| Andragogy vs Pedagogy as binary | Trainee thinks andragogy is always "better" and dismisses lectures | Discuss the spectrum concept. Use a real example where a lecture is ideal |
| Reflection without action | Beautiful Gibbs write-up that never reaches Stage 6 (Action Plan) | Ask: "What will you do differently next week? Specifically?" |
| Maslow as a rigid ladder | Trainee applies Maslow too literally and uses it to avoid engaging with learning | Discuss the flexibility of the model. Use the transcendence example |
| Bloom at the base only | All revision is memorisation — no application or analysis | Set learning objectives using Bloom Levels 3–5. Design tutorials around them |
| Kolb cycle incomplete | Lots of experience and reflection, but no active experimentation | Explicitly ask: "What will you do differently in clinic tomorrow based on this?" |
- "What would Maslow say about your motivation to learn this week?"
- "Which stage of Tuckman's model is our VTS group at right now — and why?"
- "Using Kolb, what did you actually do with the last thing you reflected on?"
- "What Bloom level was that AKT question testing — and how were you revising for it?"
Not directly — but indirectly, very much yes. The AKT has appeared with questions on educational theory, especially in the "evidence, guideline interpretation, and research" sections. More importantly, applying these principles to your own revision (spaced repetition, active recall, Bloom's higher levels) will meaningfully improve your AKT performance. And for the SCA, understanding how consultation skills are learned and practised is essential.
If you had to choose three: Knowles (so you understand what adult learners need), Gibbs or Kolb (so you can use reflection as a teaching tool), and Grow (so you match your teaching style to your trainee's needs). Miller and Bloom are equally important for understanding and designing assessments.
Kolb describes the overall learning cycle — the mechanism by which experience leads to growth through four stages. Gibbs provides a detailed structure for the reflection stage within that cycle — especially useful for emotionally complex events. Think of Kolb as the map and Gibbs as the detailed guide to one part of the journey.
No — and this is one of the most common misunderstandings. Both approaches are valid, and the choice should be determined by context. A 90-minute lecture to 150 trainees on a new NICE guideline update is perfectly appropriate pedagogy. A one-to-one tutorial exploring a trainee's professional development needs requires andragogy. The skill is in knowing which to use and when.
Start with Maslow — check whether basic needs are being met (workload, wellbeing, safety). Then consider Knowles — have you explained why this learning matters to them? Then look at Grow — are you pitching your teaching at the right level? A highly experienced IMG who is stage 4 on Grow's model will disengage rapidly from Stage 1 teaching. The mismatch, not the person, is usually the problem.
AKT High-Yield — Educational Theory in Your Revision
Every AKT question is, at its core, a clinical scenario. The best preparation connects exam content to real clinical experience — not textbook reading alone.
| Kolb Stage | What it means for AKT revision |
|---|---|
| Concrete Experience | See a patient with hypertension in clinic — or review a past case you managed |
| Reflective Observation | Review the management you used. What would the AKT say was first-line? Where did you deviate? |
| Abstract Conceptualisation | Look up the NICE guideline. Map it to a conceptual framework. Note the numbers and thresholds. |
| Active Experimentation | Do AKT practice questions on that topic — and note which answer patterns keep catching you out |
Based on Ebbinghaus's Forgetting Curve — without active review, roughly 50% of new information is lost within 24 hours and 70–80% within a week. Spaced repetition counteracts this directly.
| Bloom Level | AKT Question Type | Revision Approach |
|---|---|---|
| 1. Remember | Simple factual recall: "What is the first-line treatment for X?" | Flashcards, spaced repetition, mnemonics |
| 2. Understand | Explanation: "Why does X cause Y?" | Mind maps, summarising in own words, explaining to someone else |
| 3. Apply | Scenario: "This patient has X. What do you do?" | Practice questions, case-based revision, applying guidelines to real clinic cases |
| 4. Analyse | Comparison: "Which option is most appropriate and why?" | Comparative tables, decision frameworks, understanding why wrong answers are wrong |
| 5–6. Evaluate/Create | Complex extended matching, audit, statistics questions | Stats practice papers, QI scenario discussions, critically appraising research |
- Do not copy notes verbatim. Rewrite concepts in your own words — this forces genuine understanding
- Teach a topic to someone else (or explain it aloud to yourself). If you stumble, you have found a gap
- Connect new AKT facts to cases you have seen. The more you connect, the more you retain
- Build personal summary sheets, decision trees, and comparison tables — constructing understanding, not just receiving it
SCA High-Yield — Educational Theory in Your Consultation
The SCA tests the top half of Miller's Pyramid: Shows How (in a simulated consultation) and Does (in real supervised practice). Trainees who fail the SCA are often stuck at the lower levels — they know what to do, but cannot do it under pressure.
| Kolb Stage | SCA Preparation Activity |
|---|---|
| Concrete Experience | Run a real consultation or a role-play session with a colleague |
| Reflective Observation | Watch a recording back. Ask: Where did I lose rapport? When did I rush? Where did ICE slip away? |
| Abstract Conceptualisation | Map what happened to a consultation framework. What would you do differently? Why? |
| Active Experimentation | Do the next consultation differently — and observe what happens |
The SCA rewards trainees who have a genuine, natural consultation style — not those who have memorised a script. Constructivism explains why: you need to build your own authentic approach, not copy someone else's.
- Observe experienced GPs consulting — but do not mimic. Extract what resonates with you
- Experiment with different approaches across different patients until you find your own natural style
- Collect phrases that feel comfortable and natural to you — not phrases that feel borrowed
- Your consultation style should feel like a polished version of how you already talk to people — not a performance
Research on expert performance consistently shows that it is not the number of hours practised but the quality of deliberate practice — practising at the edge of your current ability, with immediate feedback — that drives improvement.
- Choose a specific skill to work on each week (e.g., "This week I will focus on opening consultations better")
- Run role-plays targeting that specific skill
- Get specific feedback — not "that was good" but "when you said X, here is what happened…"
- Review, adjust, repeat
- Running consultations on autopilot without reflecting afterwards
- Seeing 20 patients a day without ever asking "what did I do well there, and what could I have done better?"
- Reading consultation skills books without practising the skills
- Vague feedback that cannot be acted on
📌 Final Take-Home Points
- Educational theory is practical, not academic. These frameworks will improve your teaching sessions, your tutorials, and your exam preparation immediately.
- Andragogy and pedagogy are a spectrum — use both intelligently depending on context. Andragogy is not automatically better.
- Reflection without action is not learning — Gibbs and Kolb both require you to reach Stage 6 / Stage 4: the action point.
- Maslow first. Before expecting high-level engagement from a trainee, check that lower-level needs are being met. Sleep, safety, and belonging are not soft issues.
- Bloom's taxonomy explains why memorising facts does not prepare you well for the AKT. Aim for Levels 3–5: Apply, Analyse, Evaluate.
- Miller's pyramid explains why reading about how to consult does not prepare you well for the SCA. You must practise — with feedback.
- Grow's model: match your teaching to where the trainee currently is — not where you wish they were. Then move them forward, one stage at a time.
- Tuckman: allow groups to storm. Groups that never have a difficult conversation usually never reach genuine Performing either.
- Spaced repetition and active recall are not study tips — they are cognitive science. Build them into your AKT revision plan from day one.
- The best learning in GP training happens when all of these theories are applied together: the right environment, the right challenge, the right reflection, and the right support.
Engaging Adult Learners
How Adults Learn
Adult Learning
Androgogy, Transformational Learning & Experiential Learning
Cognitivism
Behaviourism
Constructivism
Principles of constructivism
Behaviorism, Cognitivism, Social Constructivism
Cognitive Load Theory
Androgogy
6 tips for adult learning
Adult Learning Principles
The Six Adult Learning Principles
The 3 Cs of Constructivism
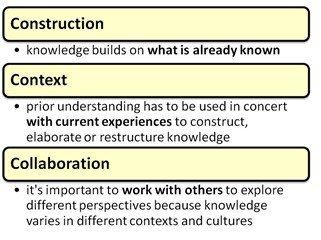
Constructivism is based on the theory that people learn best by actively constructing their own concepts, ideas and understanding usually by fitting new information together with what they already know. It’s emphasis is on the learner rather than the educator. For example, if you give a group of adults a novel to read, and then ask them to describe it, they’ll come up with their own different interpretations. Therefore, one of the most fundamental principles of constructivism is that there are no universal truths and that meaning is socially negotiated* (Duffy & Cunningham, 1996, and Windschitl, 2002). Constructivism emphasises the social nature of learning and the rich learning the group environment provides us with. It’s androgogic in nature.
Vico’s verum factum principle (1710) states that truth is verified through creation or invention and not, as per Descartes’ previously held belief, through mere observation.
Kolb's Learning Cycle (1984)

How to teach via Kolb
Motivational Theories: Maslow's Heirarchy of Needs
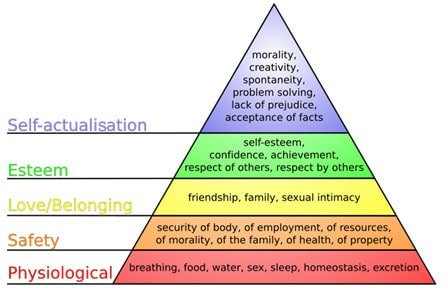
The original Maslow’s Heirarchy of Needs
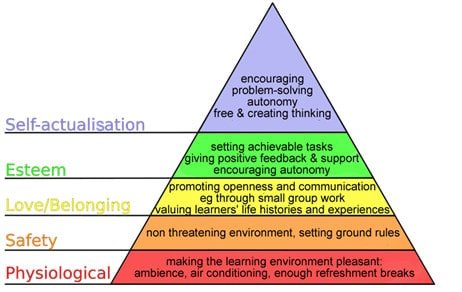
Maslow’s heirarchy applied to the classroom
(adapted from Harkin et al, 2001)