Ethnicity, Race & Culture
Because understanding your patient means understanding more than their symptoms — and because being a fair doctor is a skill you can actually learn.
A practical, honest resource for GP trainees, trainers and TPDs — covering the law, the language, the evidence, the awkward conversations, and how to handle culture in the SCA without sounding like you're trying too hard.
Much of this page is drawn from a presentation by Professor Vini Lander — Professor of Race and Education, and Director of the Centre for Race, Education and Decoloniality at Leeds Beckett University's Carnegie School of Education. Read more about her →
Downloads & Web Resources
📥 Downloads
Handouts, summaries, teaching slides and last-minute rescue revision — ready when you are.
path: Click on a folder for specific resources...
- asylum seekers - some facts.doc
- asylum seekers - the hell of being an asylum seeker.pdf
- asylum seekers and refugees - practical tips.doc
- cultural and linguistic issues plus CSA.ppt
- cultural calendar.doc
- cultural competence.ppt
- cultural diversity competence and sensitivity.ppt
- culture and health (TEACHING RESOURCE).ppt
- culture and health quiz.ppt
- culture related disease.pdf
- dddd framework - challenging unnacceptable behaviour.pdf
- diversity and culture (TEACHING RESOURCE).ppt
- ethnicity - how to use medical interpreters.pdf
- ethnicity - patterns of disease.doc
- ethnicity - south asian communities.pdf
- ethnicity - the living races and peoples of europe.pdf
- ethnicity culture and diversity.ppt
- language - do you speak english - communicating with those who speak little.ppt
- language - yorkshire slang - a glossary of terms for trainees from abroad.pdf
- racism and health - developing an interactive teaching session.pdf
- ramadan - medical conditions and fasting.docx
🌐 Web Resources
A hand-picked mix of official guidance and real-world GP training resources. Because sometimes the best pearls are not hiding in the official documents.
- The Equality Act 2010 — EHRC
- Equality & Diversity (BVTS)
- Sexuality & Gender (BVTS)
- "White Privilege" — Peggy McIntosh
- Tales of my Father — Vini Lander
- Shame vs Guilt — Brené Brown
- RCGP — Equality, Diversity & Inclusion
- GMC Good Medical Practice
- NHS Workforce Race Equality Standard (WRES)
- MBRRACE-UK — Maternal mortality reports
- John Amaechi on Privilege (video)
- Active Bystander — DDDD Framework
⏱ One-Minute Recall
- The Equality Act 2010 protects 9 characteristics, including race. Know them.
- Race, ethnicity and nationality are not the same thing. Race = physical; ethnicity = culture; nationality = country.
- Prejudice + Power = Racism. Prejudice alone is not enough.
- Unconscious bias affects everyone — even people who are genuinely egalitarian.
- Institutional racism is not about bad individuals. It is about systems that quietly disadvantage whole groups.
- "I don't see colour" is not neutral — it keeps existing power structures intact.
- The evidence is clear. Doctors from ethnic backgrounds other than White British face differential attainment in exams and GMC referrals; Black women remain around twice as likely to die during or soon after pregnancy than white women.
- The IMG shift: move from directive to shared, from clinical-only to psychosocial, from certain to honestly uncertain.
- The DDDD framework — Direct, Distract, Delegate, Delay — helps you challenge poor behaviour safely.
- Racist patients: name it, pause the consultation if needed, tell a colleague, document, report.
- In the SCA: be curious, not performative. Ask, don't assume. Meet the person, not the stereotype.
- Change starts with guilt, not shame (Brené Brown). Guilt moves us. Shame freezes us.
Why This Matters in General Practice
General practice is the frontline of modern Britain. You will see patients from every background, every faith, and every possible combination of language, culture and family structure. Your ability to meet each person where they are — without assuming, without flattening, without performing — is a core clinical skill, not a soft extra.
It also matters because the evidence is uncomfortable. BAME patients receive different investigations, different referrals, and in some cases, worse outcomes. BAME trainees face higher exam failure rates, more GMC referrals, and slower progression. If we do not talk about this honestly, we cannot fix it.
This topic feels like walking on eggshells — especially for trainees new to the UK who worry about saying the wrong thing, and for UK-trained trainees who worry about sounding insensitive. The way through is not silence. It is curiosity, humility and practice.
The 9 Protected Characteristics
It is against the law to treat someone unfairly because of any of these nine things. They are called protected characteristics, and they are shielded by the Equality Act 2010. Every GP trainee should know them.
Through the belittling, ignoring or denial of a person's identity, one can destroy perhaps the most important aspect of a person's personality — his sense of identity and who he is. Without this, he will get nowhere.— Bernard Coard, How the West Indian Child is Made Educationally Subnormal in the British School System
Our children are quietly trained into the social hierarchies around them, long before they know what they are being taught.
Race, Ethnicity, Nationality
These three words are often used as if they mean the same thing. They do not. Understanding the difference helps us speak about people more accurately — and more respectfully.
Race
Grouping people by physical characteristics, usually rooted in genetic ancestry. Race is a socially constructed idea — it was invented by societies, not biology.
Ethnicity
A group whose members share a common cultural heritage — traditions, language, history and a sense of shared identity.
Nationality
Belonging to a particular nation, usually by birth, descent or citizenship. A legal and civic status.
The word ethnic is often used as shorthand for "people who are not white." Historically, terms like BME (Black and Minority Ethnic) and BAME (Black, Asian and Minority Ethnic) have been widely used. However, the UK Government's own advice (Commission on Race and Ethnic Disparities, 2021) and many representative organisations now recommend moving away from these collective terms, as they can flatten very different experiences into one category.
There is also a simpler problem with the word minority — globally, it is just not true. Non-white people make up the overwhelming majority of the world's population. The term minority is only accurate in certain national contexts, and even then it carries a quiet suggestion of "less than" that language does not have to carry. Calling the majority of humanity a "minority" is both inaccurate and unhelpful.
On this website, we therefore use ethnic on its own — for example, "ethnic groups," "ethnic communities," "doctors from different ethnic backgrounds" — rather than "minority ethnic" or "ethnic minority". Where possible, we use the specific ethnic group instead (for example, Black African, British Pakistani, Indian).
Interestingly, the word "ethnic" comes from the Latin ethnicus, meaning heathen (Knowles & Lander, 2001). Language matters — and it keeps changing, which is a good sign.
The Danger of a Single Story
Please watch this beautiful TED talk by Chimamanda Ngozi Adichie. She explains what happens to a whole group of people when the world only hears one story about them — and how powerful it is when more stories are told.
Her talk on feminism, given from a Nigerian perspective, is also worth your time. It opens a window into the thinking of some of our trainees and trainers. Not everything transfers to the UK, but many of the unspoken cultural signals she describes certainly do.
One of her most important points is that change begins with children — and with us. Young people need to believe that more is possible for them, and that someone will support them in reaching for it. We must help people step out of the cage of pre-set ideas — that being a girl, or Black, or middle-aged and barely comfortable with computers, does not mean your life has to look a certain way.
Change has to start inside each of us. And when we see it happening around us, we need the courage to name it.
"White Privilege"
Peggy McIntosh's essay "White Privilege: Unpacking the Invisible Knapsack" is one of the clearest pieces ever written on this subject. Please read it. You will understand far more about what white privilege actually means after twenty minutes with her words than after any lecture.
Privilege here does not mean that white people have had easy lives. It means the absence of certain obstacles — not unearned riches, but unearned protection from particular hardships. The numbers below help show what that looks like in Britain.
Language in this field is evolving. Collective terms like BAME and BME were once standard but are now increasingly replaced by more specific descriptors, or by minority ethnic. The aim is to honour the real differences between communities, rather than flatten them into one grouping. When writing about individuals, use the term they use for themselves where you can.
This short video by John Amaechi gives the clearest explanation of white privilege you are likely to hear. He describes it as "the lack of impediment" rather than "unearned riches" — and he is kind about it. We all face hardship, he says, and some of that hardship comes from the absence of privileges that others are given automatically. It is not about blame or shame. It is about awareness, so we can begin to close the gap.
Notions of Deficit
The deficit theory of education used to argue that students who were different from the "norm" — in race, class, gender or ability — should be treated as deficient. The job of education, this theory said, was to correct them.
For example, by the age of five, Black children living in poverty in the UK are around a year behind their wealthy peers in vocabulary. Deficit theory would treat this as the child's problem, rather than a symptom of the conditions they were born into.
Most of us would reject this theory if it were spelled out to us plainly. But it has not fully gone. It lingers in quieter places — in the low expectations some educators hold for students of colour, or for international medical graduates. It shows up in the gentle surprise when someone "unexpected" does well. That, too, is deficit thinking.
What is Racism?
Two definitions worth sitting with:
A manifestation of hatred or contempt for individuals who have well-defined physical characteristics different from our own.— Todorov, 2009
A multifaceted social phenomenon, with different levels and overlapping forms. It involves attitudes, actions, processes and unequal power relations. It is based on the interpretation of the idea of "race", hierarchical social relations, and the forms of discrimination which flow from it.— Garner, 2010
But perhaps the single most useful way to think about racism is this:
This is important, and it is not limited to race. It applies to any group dynamic where power meets prejudice — including caste and colourism within communities of colour themselves.
If you overhear something at work, challenge it. Call it out. Racism is often reduced to a few shocking acts of aggression — but there is so much systemic material beneath the surface. That is what needs unpicking, and moving.
Unconscious Bias
Unconscious bias is about the individual, not the institution.
Unconscious biases are 'habits of mind' learned over time through repeated personal experiences and cultural socialisation. They are highly resistant to change.— Burgess et al, 2007
We gravitate towards people who look and think like us (Boliver, 2016). Burgess and colleagues put it plainly: even consciously egalitarian people may hold negative ethnic and racial stereotypes of which they may not be fully aware.
The consequence is that unintentional bias can be just as damaging as overt bias. We may not mean harm. Harm still happens.
What is Institutional Racism?
You may think racism is the fault of a few "bad apples" — and that is not you. But there is something bigger going on. There are structures built into our organisations that quietly deny fair opportunity to people from diverse backgrounds. Saying "I'm not racist, I'm not a bad apple" misses the point entirely.
The Macpherson Report, published in 1999 after the murder of Stephen Lawrence, gave us the landmark definition of institutional racism. It is still the definition we use today.
The collective failure of an organisation to provide an appropriate and professional service to people because of their colour, culture or ethnic origin. It can be seen or detected in processes, attitudes and behaviour which amount to discrimination through unwitting prejudice, ignorance, thoughtlessness and racist stereotyping which disadvantage minority ethnic people. It persists because of the failure of the organisation openly and adequately to recognise and address its existence and causes by policy, example and leadership.— The Macpherson Report, 1999
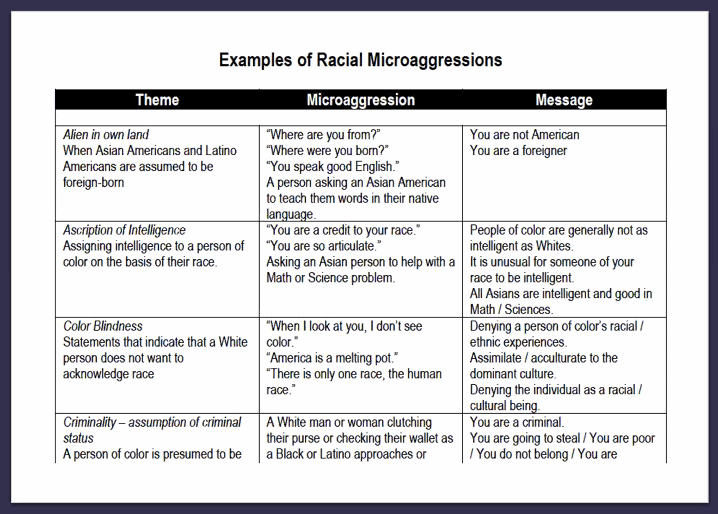
Critical Race Theory & Microaggressions
Critical Race Theory (CRT) began in American legal studies. It argues the following:
(Gilborn, 2008)
The Iceberg of Racism
A useful way to picture racism is as an iceberg. The part above the water — the overt, aggressive part — is what everyone talks about. But the much larger part sits below, quietly shaping lives every day.
Overt Racism
- Racial slurs and name-calling
- Physical attacks and hate crimes
- Explicit discrimination in hiring
- Openly racist language
Covert Racism & Microaggressions
- Mispronouncing names repeatedly
- Assumptions about competence, language or training
- "Where are you really from?"
- Being expected to speak for "your whole community"
- Tokenism and diversity-as-decoration
- Biased curricula (e.g. dermatology on white skin only)
- Unequal referral and investigation rates
- Unequal progression and promotion
- Lack of representation in leadership
- Policies that disadvantage particular groups
Colour Blindness & Whiteness
Colour blindness
"Colour blindness" is often presented as a virtue — "I don't care what colour they are. I treat everyone the same." In reality, it can be just as harmful as overt racism, because it keeps the existing power relationships intact. It sounds generous but reflects ignorance, and sometimes superiority.
When we claim not to see difference, stereotypes do not disappear — they go underground. They still shape the quiet assumptions people carry. Black children are "the ones who underachieve", or "the aggressive ones", or "the ones who are good at sport". None of that leaves the room just because we say we don't see it.
Whiteness — and moving forward
Progress is not about militancy. It is not about shame. It is about moving forward — together.
Brené Brown makes a beautiful distinction between shame and guilt. Shame says "I am bad", and it freezes us. Guilt says "I did something bad", and it moves us. We need the second, not the first.
What helps?
- Developing racial literacy — the language and knowledge to talk about race clearly.
- Working parties that include diverse voices — not as tokens, but with real power.
- Sharing pastoral work — making sure the emotional support of diverse trainees is not quietly dumped onto educators of colour.
- Scenarios and training exercises that bring trainers and trainees into the conversation together.
Injustice in the NHS — Real Examples
These are real reflections from doctors and trainees. Click each question to read the examples. They are shared here not to shame anyone, but to help us recognise what injustice and microaggressions actually look like — and to practise what to say next time.
- When I raised concerns about a senior nurse in charge, the consultant said to me: "Do you want to get along with the team, or not? I would recommend you get started by baking them treats to win them over."
- Assumptions made about a person's commitment, skills and capabilities — because they are female, less-than-full-time, from a particular country, or not trained in the UK.
- The only person of colour in our team being handed an "Embracing Diversity & Inclusivity" project as her main project to "sort out".
- Continuously mispronouncing a person's name because "it's too hard" to say correctly.
- A consultant going on a ten-minute transphobic rant when a trans patient was discussed at board round.
- A female Pakistani colleague being verbally abused by an older white patient with dementia. The work was important so she felt conflicted about removing herself. Everyone else just put it to one side — "it can't be helped, she has dementia" — without thinking about the colleague.
- How to challenge a cleaner who uses racist language — hard to challenge without "punching down".
- A GP partner saying, "Oh no, I hope this isn't going to be another difficult trainee" — when the name of the next trainee (a non-English name) was mentioned.
- Worried that I would make it worse. That's why I didn't say anything. I felt bad that I didn't.
- I have been worried about challenging hierarchy and authority, especially when the microaggression comes from a consultant.
- I raised it with another consultant.
- I felt awful when my own microaggressions were pointed out. I had to own it — by apologising and learning.
- I said: "Can I just say, not all IMGs are bad trainees. A lot of them are so good, just like those who trained here. Remember, they wanted to do medicine, so their hearts are in a good place. Let's not judge them before they've started, otherwise we'll fulfil our own prophecies." They all agreed — but I wonder if I could have said it more kindly, rather than "outing" the people who were microaggressing. Sometimes I get so passionate that I speak with passion, and it can come across as aggression. When something touches a core value of mine, I find it hard to control my tone and volume.
- I have sometimes called them out — mainly when it comes to sexism.
- "What do you mean by that?"
- "I'm sure you didn't mean it, but that sounded a bit like you were saying xyz."
- "I get what you mean, but I wonder if there's a different way to say that?"
- "Come on, don't be like that — they're just trying to help you."
- "It's not like you to say something like that. Do you know how it sounded? Is there something going on that makes you say that?"
- Consider the context. If it is clear racism or anti-LGBTQ — call it out. If milder, say it more mildly but clearly. In both cases, say it with kindness and compassion — the person is more likely to embrace change than defend themselves.
- Consider the situation. One-to-one conversations usually land better than calling someone out in a ward round or meeting.
- Consider the timing. Say something as soon as possible after the incident — but when there is space for both people to talk. For example, after the ward round, not during it. That may lead the consultant to acknowledge the moment at the next ward round, making it clear to the rest of the team that the issue was not overlooked.
The DDDD Framework
When you witness poor behaviour, it can be hard to know what to do in the moment. The DDDD framework — from the Active Bystander programme — gives you a simple sequence of steps. It helps you challenge unacceptable behaviour in a way that opens the door to change, rather than shutting it.
The beauty of DDDD is that you always have at least one option available, even when the others feel too risky. The aim is not to win an argument. The aim is to reinforce, gently but firmly, where the line is.
But Talking About Race Feels Like Walking on Eggshells
Yes. It does. And we need to breathe through that discomfort, because how else do we get to the other side? Tackling inequality is everyone's responsibility.
Peggy McIntosh offers a helpful image. She says she was born into a white, privileged background — and it is like being handed a bank account with money in it, without asking for it. What she chooses to do with that account is her responsibility. She can use it to reduce the inequalities around her.
We cannot be complicit in maintaining the inequalities that exist in our society. Each of us, when we do nothing, is contributing. When we do nothing, we sustain the gap.
It is easier to stay with people who feel familiar — birds of a feather flock together, as the saying goes. That is unconscious bias at work. We don't look because we are not the ones causing harm directly. But we are complicit the moment we look the other way.
You may see yourself as not racist. You don't hurl abuse. But there are things life has given you that others have not been given — simply because of where and how you grew up. Most of us end up where we are not purely through merit. Many of us were given a quiet head start, at the expense of people from different backgrounds who were never given the same. That is the inequality we are talking about.
Sit with the discomfort. This is what people of colour face every day.
And remember: shaming and blaming is not how change happens. Change happens through compassion, dialogue, discussion, forgiveness and love.
Racial Inequalities in Medicine & Healthcare
This is not abstract. The effects of racism in medicine are measurable, and they are measured. Here is a selection of what the evidence shows.
For doctors and students in training
For patients
Other things worth knowing
- Medical students from ethnic backgrounds other than White British are less likely to get a First or Upper Second class degree. There is an attainment gap that runs from medical school through to postgraduate exams.
- Doctors from ethnic backgrounds other than White British apply for more posts on average than White doctors to reach the same outcomes — and are less likely to be shortlisted or appointed (GMC data).
- Doctors from ethnic backgrounds other than White British are more likely to be referred to the GMC by employers. The GMC has acknowledged this disparity and committed to reducing it in its published Fair to Refer? and follow-up programmes.
- There is limited ethnic diversity in medical research — most study participants are white, which has implications for the evidence base.
- Dermatology has historically been taught predominantly on white skin. Textbooks and teaching resources are slowly being updated, but the gap remains.
- The higher you climb the medical hierarchy, the whiter the room tends to become — particularly at consultant, partner and board level.
- Racist abuse still happens — from patients and from colleagues — and is now recognised formally in BMA, GMC and NHS England guidance.
- Ethnicity data is often missing from records of disease and death, which makes inequalities harder to see and harder to act on.
- The question of how NHS services are experienced by ethnic communities beyond the White British majority — and whether they feel listened to — is still not asked often enough.
Differential Attainment — What the Data Shows
"Differential attainment" is the term for the gap in exam and progression outcomes between different groups of trainees — a gap that persists even after controlling for other factors. The numbers below come from UK primary care research and the General Medical Council. They are uncomfortable. They are also the starting point for change.
exam pass rates the pattern
-
Highest pass rates
UK-qualified white doctors have historically had the highest first-attempt pass rates across MRCGP assessments.
-
Lower pass rates
UK-qualified doctors from ethnic backgrounds other than White British, on average, have lower first-attempt pass rates than their White UK-qualified peers.
-
Lowest pass rates
International medical graduates have historically had the lowest first-attempt pass rates — though the gap is narrowing with targeted national support programmes.
Source: General Medical Council and RCGP data, summarised across multiple BJGP analyses (e.g. Woolf 2019; Esmail & Roberts 2013). Specific percentages vary by year and exam diet — check GMC/RCGP annual reports for the latest figures.
Why does the gap exist?
The research is clear on one point: the gap is not explained by ability. After controlling for A-level results, school type, socio-economic status, parental occupation, language, motivation, study habits and personality, a difference remains. The causes are multiple and structural:
- Relationships matter. BME trainees describe feeling they have to work harder to prove themselves, and finding it harder to get support from senior colleagues when things go wrong.
- Isolation is real. UK qualitative research finds trainees from minority backgrounds can feel more isolated, especially when there is a difficulty with the trainer themselves.
- IMGs face a steeper induction. Cultural and consultation-style differences, unfamiliar NHS systems, separation from family, and a learning culture that rewards assertiveness all add up.
- Unconscious bias shows up in workplace-based assessment. Less well-evidenced than exams, but harder to audit — and where much of the quiet gap lives.
- The deficit framing still lingers. Educators sometimes see "at risk of failing" trainees through a lens of what they lack, rather than what the system is not giving them.
What is being done
Since 2020, a national response has taken shape. NHS England, NHS Education for Scotland, the RCGP and the GMC have launched a coordinated programme — and outcomes are already improving where targeted support has been offered:
Five task groups
Covering awareness, education, professional development, external stakeholders, and representation — reviewing the MRCGP curriculum and exam design.
Targeted support programme
NHS England has offered individualised support to previously-unsuccessful trainees — including help with exam readiness, NHS induction, and local language. Programme evaluations report markedly improved completion rates.
Built-in bias reduction
The SCA replaced the CSA/RCA in 2023 with bias-reduction work built into case design, role-player casting and wording. More attempts are now permitted (six, matching other specialties).
From deficit to difference
Educational supervisors are being trained to recognise bias in themselves and in assessment processes. The narrative is shifting from "can't do" to "must do".
The gap is real, but it is not your verdict. Thousands of IMG and BAME doctors pass each year and go on to become excellent GPs. The numbers are a reason to seek out targeted support early — from your deanery professional support unit, your TPD, peer study groups and mentoring schemes — not a reason to doubt yourself.
The GP Action Framework
Understanding race and culture is one thing. Putting it into practice in your consulting room is another. Here is a simple, usable sequence for every consultation.
Meet the person, not the label
Start every consultation with curiosity. Do not decide who this person is before they have spoken.
Ask about their world
Who is at home? What do they believe? What worries them most? Language, faith, family structure — ask, don't guess.
Notice bias in your own thinking
Am I making assumptions about compliance? About intelligence? About family roles? Pause and check.
Adapt the management, not the relationship
Adjust medication timing in Ramadan. Offer interpreters. Consider family dynamics. Stay warm and consistent throughout.
Check understanding before closing
Especially where English is a second language. Ask them to summarise the plan back to you.
Safety-net and document clearly
Include cultural and communication considerations in your notes. Future clinicians benefit from your context.
Handling a Racist Patient
Racism from patients towards doctors and staff from different ethnic backgrounds is not rare. Successive NHS Staff Surveys have consistently shown significant proportions of staff from different ethnic backgrounds reporting discrimination from patients, relatives or members of the public. The good news: there is a clear, sanctioned pathway, drawn from BMA, GMC and NHS England guidance. You do not have to figure this out alone.
Name it in the moment — calmly, clearly, without a lecture
A short, steady sentence does more than a long explanation. You are drawing a line, not opening a debate.
Pause the consultation if the behaviour continues
If the patient does not stop, you are allowed to pause or end a non-urgent consultation and offer to rebook with clear expectations. This is supported by GMC Good Medical Practice (2024), the BMA, and NHS England zero-tolerance policies. Always balance this with your duty of care — if the patient has an urgent clinical need, that must still be met safely, either by you or by a colleague.
Tell a colleague and your trainer — the same day
Do not sit with it alone. Being told "I just laughed it off" by a colleague is one of the most painful parts of this experience for many trainees. Speak to someone. If your trainer is not available, use your TPD, your educational supervisor, or the deanery lead for cultural safety.
Document clearly in the notes
Factual, non-emotive language. What was said, in whose words, your response, the outcome. This protects you, future clinicians, and — if needed — the disciplinary trail. Keep a personal note of the date, time, witnesses and any incident number too.
Report through the practice zero-tolerance pathway
Most NHS organisations have a staged process for managing unacceptable patient behaviour — typically starting with a formal warning letter and, if the behaviour is repeated, leading to potential removal from the practice list. Your practice manager, GP partners and LMC can support this. BMA guidance (Managing discrimination from patients and their guardians/relatives, 2022) sets out the principles in detail.
Look after yourself afterwards
Reach out to the BMA wellbeing service, your deanery professional support unit, or Practitioner Health. This is not weakness — it is the same aftercare you would urge on a colleague. Racism from patients carries a psychological cost, and that cost deserves addressing, not minimising.
Do not refuse to treat a patient because of their ethnicity — this is a disciplinable GMC matter under Good Medical Practice (2024). The pathway above exists for handling abusive behaviour from a patient, which is different in kind. A patient has no right to choose their clinician on the basis of ethnicity, and equally a doctor may not withhold care on that basis.
When racism happens to a colleague and you are in the room, say something. Even a short "that's not okay" in the moment is enormously powerful. The most corrosive part of racist abuse for targets is colleagues who stayed quiet. Silence reads as agreement. Use the DDDD framework earlier on this page as your guide.
The IMG Consultation Shift
If you trained outside the UK, your consultation style was almost certainly shaped by a different system — one that was entirely appropriate for where you practised. UK general practice asks for something different, and the SCA is built around that different expectation. The table below captures the most common adjustments trainees describe having to make.
UK GP trainee communities consistently flag the same handful of "consultation-style shifts" — patterns that trip up IMG candidates again and again. These are not about language or knowledge. They are about expectation. Spotting the shift is usually enough to start making it.
The "Broken Mirrors" story — a cautionary tale
Not all adjustment advice is good advice. Sometimes trainees are told, in the name of "improving communication", to change something they should never have to change. The following is a real, published case from UK general practice — and it is essential reading for trainers as well as trainees.
A Black male trainee, told to "shrink" in white patients' consultations
A tall Black male GP trainee was observed consistently adopting a physically subordinate posture when consulting white patients — almost, his trainer wrote, "like a servant bowing before their master." When gently asked why, he explained that a previous (white) trainer had told him that his build (he is 6 feet tall) would be "overwhelming and could instil fear in white patients." He was advised to avoid mirroring the patient, and to make himself physically smaller in the consultation.
He took this on board, embarrassed and keen to improve. He did not raise it with anyone — trainees rarely raise concerns like this, for fear it will affect their career. He spent months consulting in a shrunken, apologetic posture he never should have been asked to adopt.
Mirroring is a powerful communication skill — but it works both ways. A trainee should never be coached to diminish their own physical presence, identity, or voice to make a patient "more comfortable". That is not feedback. That is racism dressed as teaching. Feedback must build the trainee up, never shrink them down.
If feedback you have received feels like it is asking you to disappear rather than improve, trust that feeling. Good feedback helps you become more yourself as a clinician — not less. Raise it with another trainer, your TPD, or your deanery lead. You are not being difficult. You are being well-trained.
Insider Pearls — What Nobody Tells You Early
The following insights come from recurring themes across UK GP trainee blogs, training forums, deanery newsletters, and UK GP training YouTube content. They are the kinds of things experienced trainees wish someone had told them in ST1. Each one has been checked against RCGP, GMC and NICE guidance before being included here.
Change one phrase at a time
Trying to overhaul your whole consultation style at once backfires — you end up stilted and self-conscious in clinic. The advice that comes up again and again: pick one new phrase, try it in every second consultation for a few days, then add the next. Slow stacking works.
Video yourself weekly — even when it hurts
UK GP training videos repeat this advice constantly: watching yourself on video reveals habits you won't notice any other way — interrupting, looking away at the screen, racing through ICE. Five minutes of honest self-review beats an hour of reading a textbook.
Don't over-apologise for your English
Many IMGs start with "Sorry, my English is not perfect…" — which is gracious, but unnecessary, and subtly undermines you before the consultation has even begun. Your English is a working clinical tool. Just consult. If the patient asks you to repeat, repeat. No apology required.
Role-play in threes, twice a week, for three months
The pattern trainees who pass first time describe most often: a study group of three (doctor, patient, examiner — rotating roles), meeting twice a week for around three months before the exam. Not an hour of reading. An hour of doing. This is the single highest-yield preparation strategy.
Ask the patient to summarise the plan back
The simplest check-understanding technique, and one of the most under-used. "Just so I know I've explained it clearly — would you mind telling me what you understood?" It is respectful, it catches misunderstandings before they become problems, and examiners love it.
Layered reflection beats simple paraphrase
Instead of "So the pain is constant", try "You're saying the pain is constant, and that's leaving you feeling exhausted and a bit hopeless." Layered reflection names content and emotion together. It signals you are listening in full — not just hearing words.
Asking ICE as a tick-box
Trainees learn "ideas, concerns, expectations" and then fire all three questions at the patient in the first 90 seconds, robotically. It sounds exactly as awkward as it reads. Weave ICE into the conversation naturally — "What were you thinking it might be?" after a pause, not after introducing yourself.
Practise with an 8-minute timer
A widely-shared pre-exam tip: practise consultations under an 8-minute constraint rather than the full 12. When you return to 12 minutes on exam day, it feels spacious. The same principle distance runners use — train harder than the race.
Use the 3 minutes of reading time properly
Before each SCA case, you get three minutes with the notes. Forum consensus: use this to mentally rehearse your opening sentence, a likely working diagnosis, and two management options. Do not just read passively. You are building the scaffolding you'll consult on.
Don't outsource your decision to ARRS
"I'll refer you to the pharmacist / social prescriber / physio" — without doing any clinical management yourself — reads as unsafe. Referral is an addition to your plan, not a replacement for it. Apply NICE guidance, make a decision, then add the referral if it helps.
Controlled silence is a skill
After a probing question, count silently to three before filling the gap. Most trainees find this uncomfortable — which is exactly why it works. Patients often reveal their deeper concern in that tiny pause. Examiners notice the restraint.
Meta-communication — talking about the talking
A subtle, high-scoring move: "I notice you pause when we talk about insulin — would it help if I explained more slowly, or used a diagram?" You're showing the patient you're tuned in not just to the words, but to how the conversation is landing for them.
Don't avoid interpreters in clinic
Trainees sometimes try to "get through" consultations with broken English rather than book an interpreter, worried about time. This is a safety issue. Always offer an interpreter where language is a barrier — and document the offer. The SCA will test this. Real practice expects it.
Your FourteenFish ePortfolio is not optional
Many IMGs over-invest in AKT and SCA preparation, and under-invest in the portfolio. WPBA is one of the three required components of the MRCGP alongside the AKT and SCA — and all three must be satisfactory for CCT. A strong exam performance cannot rescue a thin portfolio at ARCP. Keep it current throughout the year, not in a panic before panel.
If there is one insight that comes up across every UK GP training forum, blog and video channel, it is this: the SCA is about performance, not knowledge. Reading about consulting will not get you through it. Practising, being watched, receiving feedback, and changing — will.
🎯 Embracing Culture, Race & Ethnicity in the SCA
In the SCA, cultural awareness matters — but it has to feel real. Examiners (and patients) can sense when it is performed rather than meant. Here is how to get it right without tipping over into the awkward or the tokenistic.
Treat the patient as an individual first
Start from who this person is, not what group you assume they belong to. Culture is one thread in their story, not the whole story.
Ask — don't assume
Open, humble, patient-led questions let them tell you what matters. You never need to guess.
Notice — without announcing
If a patient mentions Ramadan, a family elder, or a community pressure, take it on board naturally. You do not need to say "how interesting" or flag that you've noticed.
Adapt the plan, not the performance
Culture should change how you manage — timing of medication in Ramadan, involving family in a decision — not how loudly you identify with them.
Check language, don't assume fluency
If English may not be their first language, check understanding gently. Offer an interpreter where needed. Never raise your voice — slow and clear is kinder and better.
Be humble when you don't know
"I'm not sure I understand the significance of that for you — can you help me?" is a strong, safe phrase. Examiners reward honest curiosity far more than false familiarity.
🗣 Useful SCA phrases for cultural moments
- "Is there anything about your background, beliefs or home life that would help me understand how best to help you?"
- "Who at home do you usually talk to when you're making big decisions about your health?"
- "I want to make sure this plan works with how you live — is there anything you'd like to change or adapt?"
- "Would it help if we planned your medication around Ramadan?"
- "I'm not sure I understand the significance of that for you — can you help me?"
- "I want to get your name right — could you say it for me?"
Getting the tone right — do & don't
Cultural awareness in the SCA is not a box to tick or a performance to deliver. It is simply good, attentive, humble medicine — meeting the person in front of you, not the group you think they represent.
Teaching This Topic — Trainer Pearls
Race, ethnicity and culture are not easy topics to teach. Trainees may feel defensive, anxious, or unsure what is safe to say. Your job is to make the conversation possible — not perfect.
🎯 Tutorial starters
- Watch the Chimamanda TED talk together, then debrief
- Use the DDDD framework with a real-life workplace scenario
- Ask: "What was the last time you felt you got culture right — or wrong — in a consultation?"
- Role-play the "Nigerian friends too" moment, then try again better
⚠ Common trainee blind spots
- Assuming IMGs will "get" UK cultural nuance without teaching
- Assuming UK-trained trainees don't need this teaching
- Confusing "being polite" with "being culturally aware"
- Missing the difference between overt and covert racism
- Not knowing how to handle patient racism towards colleagues
💡 Reflective questions
- When did you last consult across a real language barrier?
- Whose name have you quietly avoided saying because it felt hard?
- What assumption did you catch yourself making this week?
- Where in your practice is the patient demographic under-served?
🩺 Case scenarios for tutorials
- Patient with dementia using racist language toward a colleague
- Teenage girl attending with mother — consent & confidentiality
- Man asking for his wife's test results "on her behalf"
- Ramadan consultation with a newly diagnosed diabetic
- Interpreter not available — how to proceed safely
Consider building this into your VTS programme as a thread, not a one-off. A single session can raise defences. A consistent, low-pressure series builds genuine racial literacy over time — and lets you spot which trainees (and trainers) need extra support.
✦ Final Take-Home Points
- The 9 protected characteristics are the legal backbone. Know them by name.
- Race, ethnicity and nationality are three different things. Use them with care.
- Prejudice + Power = Racism. Racism needs power behind it — which is why it is a systemic problem, not just a personal one.
- Unconscious bias affects everyone — including people who believe they are fair. Good intentions are not enough.
- "I don't see colour" is not neutral. It maintains the status quo.
- The evidence is real. Trainees from ethnic backgrounds other than White British face differential attainment. Doctors from these backgrounds are also referred to the GMC at higher rates. Black women remain around twice as likely to die during or soon after pregnancy than white women. These are facts.
- DDDD — Direct, Distract, Delegate, Delay — gives you a way in when you witness poor behaviour.
- In the SCA: be curious, not performative. Ask, don't assume. Meet the person, not the group.
- Guilt moves us. Shame freezes us (Brené Brown). Choose guilt, choose action, choose change.
- Sit with the discomfort. This is what people of colour face every day. Your discomfort is where growth begins.
Some videos worth watching
Our children are unconsciously trained into our social heirarchies.
Don’t think for one second that our children are blind to colour and race.
“Through the belittling, ignoring or denial of a person’s identity, one can destroy perhaps the most important aspect of a persons personality, his sense of identity and who he is. Without this, he will get nowhere.”
From “How the West Indian Child is Made Educationally Subnormal in the British School System” by Bernard Coard.