Debriefs in GP Training
📥 Downloads
Useful downloads for learning, teaching, or last-minute rescue revision.
Templates, learning needs logs, and our popular guide to getting your head around debriefing — all ready to use.
path: DEBRIEFS
Identifying Learning Needs — From Real Surgeries
A full toolkit of learning needs logs drawn from real GP consultations — baby clinics, general surgeries, video analysis, sit-and-swap sessions, and more.
path: IDENTIFYING LEARNING NEEDS - from real surgeries
- debrief template.doc
- debriefs - learning needs log.docx
- debriefs template for recording learning.doc
- getting your head around debriefing.pdf
- learning needs log from baby clinic.docx
- learning needs log from general daily practice.docx
- learning needs log from interesting patients.docx
- learning needs log from random case analyses.docx
- learning needs log from sit n swap surgeries cot style.docx
- learning needs log from sit n swap surgeries csa style.docx
- learning needs log from sit n swap surgeries.docx
- learning needs log from video analysis - cot crib.docx
- learning needs log from video analysis.docx
🌐 Web Resources
A hand-picked mix of official guidance and real-world GP training resources. Because sometimes the best pearls are not hiding in the official documents.
📖 What Is A Debrief?
The Definition
A debrief is a dialogue between two or more people — usually a GP trainer and a trainee — about a real patient situation that has already occurred.
Its goals are to:
- Discuss the actions and thought processes involved in a specific patient case
- Encourage reflection on those actions and processes
- Explore how future performance might be improved
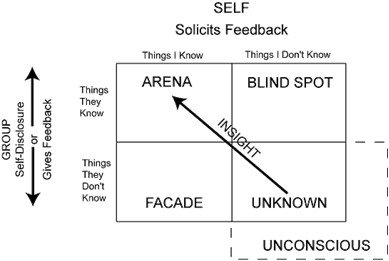
🔍 Johari's Window — The Educational Heart of Debriefs
In debriefs, you are trying to reach and explore the blind spot — the things the trainee does not know about themselves. Johari's Window, developed by psychologists Luft and Ingham, maps what is known and unknown to self and others.
A great debrief is a structured, compassionate opening of the blind spot.
Trainees often genuinely do not know what they do not know. A trainee who under-investigates, over-prescribes, or consistently misses the psychosocial story cannot fix what they cannot see. The debrief makes the invisible visible — respectfully, repeatedly, and over time.
🎯 The Two Purposes of Debriefs
Trainees are still learning. You must ensure that no patient has been harmed, or is at risk of harm, from what the trainee did (or did not do) in that consultation.
Every patient is a learning opportunity. Once safety is confirmed, the debrief becomes a tutorial — exploring knowledge, skills, and attitudes in real clinical context.
Safety always comes first. Educational depth is valuable — but never at the expense of checking that the patient is safe. This is especially critical for ST1 and ST2 trainees who are not yet ready for independent practice.
⚡ Quick Summary — If You Only Read One Thing
The Debrief in 60 Seconds
- A debrief is a structured conversation between trainer and trainee about real patients seen in clinic
- Primary purpose: Patient safety — ensure no patient has come to harm
- Secondary purpose: Education — help the trainee grow
- ST1/ST2: review every patient every session — they are not ready for independent practice
- ST3 (early): still review all patients; ease off gradually as independence grows
- Debriefs are mandatory — they must be timetabled and protected
- Use KSA + Bloom's Taxonomy + RCA style to add educational depth
- The biggest mistake: letting a debrief drift into a chat — push for challenge instead
- If you advise action, document it in the patient record — protect yourself legally
- Debriefs feed directly into AKT knowledge and SCA consultation skills — use them strategically
🌟 What Good Debriefs Achieve Over Time
When debriefs are done well and consistently, the cumulative effect on a trainee is significant. These are not abstract educational goals — they are the practical changes you should see over months of good supervision.
- Trainers and the practice can be confident patients are not being exposed to avoidable harm
- Patients get the reassurance — even if unconsciously — that their consultation has been reviewed by a senior doctor
- Trainees develop the metacognitive awareness to reflect on their own practice independently
🏥 Debriefs by Stage: ST1/2 vs ST3
ST1 & ST2
- Review every patient, every session — no exceptions
- Not ready for independent practice at this stage
- Include telephone consultations in the review
- Put measures in place to cover home visits
- Encourage the trainee to ask: "Would you mind debriefing my home visit?"
- Once safety is confirmed, move to the educational discussion
- Group debriefs with other FY2 or GP trainees can work very well
ST3
- Early ST3: still review every patient — beginning of their final year, not yet independent
- Mid ST3: as competence grows, selective review is acceptable — spot-check random patients
- Late ST3: transition to autonomous practice, but maintain a supervising GP for each session
- Concerns about clinical ability? Return immediately to reviewing every patient — regardless of stage
- Consider themed debriefs for able ST3s (e.g. prescribing only, or referrals only)
⚠️ Note on SCA timing: ST3 trainees planning an early SCA should move to shorter appointment slots faster — factor this into timetable planning early in the year.
Appointment Length Guidance by Stage
| Stage | Period | Appointment Length | Debrief Frequency | Notes |
|---|---|---|---|---|
| ST1/ST2 | First 4 weeks | 30 minutes | Every patient + 30 min end-of-session | New to GP — IT, admin, and clinical all unfamiliar |
| ST1/ST2 | Months 2–4 | 20 minutes | Every session — 30 min debrief at end | Building confidence and speed |
| ST1/ST2 | Remainder | 15 minutes | Every session — 30 min debrief | Consolidating clinical reasoning |
| ST3 | First 4 weeks | 20 minutes | 10 min per patient initially | Even ST3s need careful initial assessment |
| ST3 | Weeks 5–8 | 15 minutes | Every 2–3 patients | Growing independence |
| ST3 | Mid-placement onwards | 10 minutes | 30 min end-of-session debrief | Near-independent; supervising GP available but not reviewing all |
These timings are suggestions, not rules. Tailor to the individual. A trainee who has recently done a GP placement in ST2 may progress faster. One who is struggling clinically needs to slow right down — regardless of what the calendar says.
🗓 Slotting Debriefs into the Timetable
Debriefs do not happen by accident. They need to be planned, protected, and timetabled in advance. A debrief squeezed into a gap between your own patients is a debrief that will get cut short when your next patient runs over. That is a patient safety risk.
- Agreed periods of protected debrief time must be built into the timetable before the trainee starts
- Debriefs are mandatory — they are not optional extras
- The debrief doctor does not have to be the GP Trainer — share the load across the whole team
- Make sure the debriefing doctor knows they are debriefing that session
- Consider an annual in-house teaching session on "how to debrief well" — include refreshers for experienced staff and training for new doctors
🔧 How to Do a Debrief — The Traditional Approach
For each patient reviewed, work through these domains in a structured way. The power of this approach is that even the most straightforward-looking case can reveal rich educational material when you pull at the right threads.
The Core Review Domains
| Domain | What To Ask / Explore | Why It Matters |
|---|---|---|
| Data Gathering | Was enough history taken? Were important symptoms explored? What was missed? | Drives diagnosis accuracy; directly tested in AKT and SCA |
| Diagnosis & Reasoning | Was the diagnosis reasonable? Was differential diagnosis considered? How was uncertainty managed? | Core professional capability — DD (Decision-Making and Diagnosis) |
| Investigations | Were investigations appropriate? Over- or under-investigated? Results interpreted correctly? | Common AKT topic; important for patient safety |
| Clinical Management & Prescribing | Was the management plan evidence-based? Prescribing safe and appropriate? Safety-netting done? | CM capability; heavily tested in AKT |
| Communication Skills | Did the trainee explore ICE? Was the explanation clear? Was the patient genuinely heard? | SCA marking domains directly reflect this |
| Working with Colleagues | Was appropriate help sought? Referral decisions sound? Escalation appropriate? | TW (Team Working) capability |
| Record Keeping | Are the notes adequate? Narrative clear? Red flags documented (even absent ones)? Minimum clinical data recorded? | Medico-legal importance; often overlooked by trainees |
Experienced trainers always check whether the trainee has documented the absence of red flags — not just their presence. "No weight loss, no haematuria, no night sweats" in a note is powerful evidence of a safety-conscious consultation. Trainees who only write what was positive leave themselves exposed.
✨ Adding Spice to Debriefs
A good debrief uses the basic safety-and-education framework as its foundation — but the best debriefs go further. Here are six ways to transform a routine debrief into something genuinely memorable.
For each patient, consciously ask yourself: is this a knowledge gap, a skills gap, or an attitudes gap? The answer changes how you teach.
| Type | Example | Best Response |
|---|---|---|
| Knowledge | "I didn't know the NICE CKS first-line for UTI in pregnancy was nitrofurantoin" | Signpost to NICE CKS. Set homework. Ask them to present it next week. |
| Skills | "I found it hard to structure the consultation when the patient had three problems" | Roleplay the scenario. Practice prioritisation phrases. Use RCA. |
| Attitudes | "I felt the patient was just drug-seeking so I didn't explore further" | Explore the assumption. Discuss bias. Reflective exercise or log entry. |
Use Bloom's six levels to shape how deeply you challenge the trainee on a given topic. Don't always stay at the bottom two levels.
| Bloom's Level | Sample Debrief Question |
|---|---|
| Remember | "What is the first-line antibiotic for a simple UTI?" |
| Understand | "Why do we avoid trimethoprim in early pregnancy?" |
| Apply | "This patient is 10 weeks pregnant. What would you prescribe?" |
| Analyse | "What factors made this case more complex than a routine UTI?" |
| Evaluate | "If you had that consultation again, what would you do differently and why?" |
| Create | "How would you design a safety-netting approach for patients with recurrent UTIs on your list?" |
Most trainers naturally stay in the lower three levels. The educational magic happens in the top three — particularly Evaluate and Create. More on Bloom's here.
This is where debriefs go from good to outstanding. Once you have reviewed what actually happened, start changing the scenario.
- "What if she had had double vision with her headaches — what would you have done then?"
- "What if the patient had been 10 years older and on warfarin?"
- "What if he had refused the referral?"
- "What if this was a 9-year-old rather than a 50-year-old?"
- "What if the bloods had come back abnormal?"
This is deliberate creation of cognitive dissonance — the mental discomfort of having your assumptions challenged. That discomfort is the learning happening in real time. More on RCA here.
Debriefs do not have to be one-to-one. Group debriefs — with other FY2 doctors or GP trainees — multiply the educational impact. Peers often challenge each other in ways a supervisor cannot.
- Shared debriefs are particularly valuable for junior trainees — they see a range of approaches and normalise their own experiences
- Peers can ask questions the trainer did not think to ask
- Social learning — hearing that others made the same mistake is genuinely reassuring
- Also creates accountability — you prepare more carefully if peers will hear the case
Use your VTS Half Day Release session to run occasional group debriefs. Pick three or four cases from that week — one from each trainee — and discuss as a group with the trainer facilitating.
For the very able ST3 trainee who is clearly approaching independent practice, themed debriefs can add real depth without repeating the same review format each time.
- Prescribing audit: Look only at the prescribing decisions for that session. Were they evidence-based? Appropriate dosing? Drug interactions checked?
- Referral review: Was each referral necessary? Was the right specialty chosen? Was it the right urgency?
- Investigations theme: Look only at blood tests and investigations ordered. Appropriateness, timing, follow-up plans.
- Record keeping focus: Review the quality of notes only. Completeness, narrative, red flag documentation.
- Communication skills: For each patient, how well was ICE explored? How was uncertainty communicated?
- Safeguarding lens: Were there any safeguarding concerns in the list? Were they recognised and acted upon?
Assessment drives learning — this is one of the most well-established principles in medical education. During debriefs, explicitly connecting a clinical point to its AKT or SCA relevance is not "teaching to the test." It is helping the trainee understand why this knowledge matters at the level examiners expect.
"This question about the UTI treatment — do you know how the AKT would frame this? They love threshold questions. What is the prescribing rule in pregnancy? In the elderly?"
"In your SCA, the actor would have been quite worried here. How would you have explored their concern more explicitly? What phrase could you use next time?"
See the full AKT & SCA sections below for a comprehensive list of how debriefs drive exam success.
🏋 Trainer Skills for a Great Debrief
If you can run a good consultation — and 99.9% of GP trainers can — then you already have the fundamental skills to run a good debrief. The consultation skills you use with patients translate directly: listening, picking up cues, asking open questions, negotiating, and empathy. Use them on your trainee.
Core Facilitation Skills
- Actively listen — do not prepare your next question while they are talking
- Seek clarification before making assumptions
- Pick up on verbal and non-verbal cues — is the trainee stressed? Disengaged? Overconfident?
- Elicit ideas, thoughts, concerns, and feelings — yes, these matter in a debrief too
- Negotiate future actions rather than issuing orders
- Help the trainee build self-knowledge of their own strengths, weaknesses, and attitudes
Identifying Learning Needs
- Think in terms of the RCGP curriculum — what do they need to work on?
- Think in terms of the 13 Professional Capabilities — which ones are showing gaps?
- Some learning needs can be addressed immediately in the debrief itself
- For deeper topics, set homework or plan future tutorial sessions
- Negotiate — do not just assign tasks; agree on them
Practical Tips
- Ask about urgent concerns first — what is the trainee most worried about from today's list?
- Move away from being the Expert — your job is to facilitate thinking, not to deliver lectures
- Get them to problem-solve — resist the urge to give the answer immediately
- Promote "looking it up" rather than always providing the answer — build the habit of evidence-seeking
- If in a group: open questions out to others — do not let the conversation stay between you and one person
- Some questions need direct answers: do not turn everything into a Socratic exercise — sometimes they just need to know the answer
- Balance telling, asking, and exploring — the best debriefs use all three
- Watch the time: if a trainee is verbose, redirect compassionately — "Sorry to cut things short, but…"
Tackle one or two learning needs in depth. For the rest, signpost to guidelines and resources and let the trainee follow up independently. This is not laziness — it is teaching. The trainee who learns to find the answer themselves is more independent than one who waits for the trainer to provide it every time.
⚔ Chat vs Challenge — The Most Important Distinction in Debriefing
This is the single biggest difference between a debrief that changes a trainee and one that does not. Most trainers naturally drift towards the chat end of the spectrum — it is warmer, more comfortable, and feels kind. But it produces far less learning.
💬 Chat
- Comfortable and warm
- Trainer does most of the talking
- Stays at a surface level
- No cognitive dissonance created
- Trainee leaves feeling reassured but unchanged
- Educational impact: low
🎯 Challenge
- Slightly uncomfortable — in a good way
- Trainee does at least 50% of the talking
- Pushes into the unknown — "what if" questions
- Deliberately creates cognitive dissonance
- Trainee leaves thinking differently about their practice
- Educational impact: high
Challenge means pushing people to think. It does not mean making them feel stupid, undermined, or anxious. A trainee should leave a challenging debrief feeling slightly stretched but genuinely supported. The aim is never to destroy — it is to create growth. The skill is finding that line and staying on the right side of it.
What is Cognitive Dissonance?
Cognitive dissonance is the mental discomfort that arises when a person's existing beliefs are challenged by new information. In learning terms, it is the experience of realising: "I thought I knew that — but actually I don't." That moment of discomfort is productive: it motivates the brain to resolve the tension, and resolution means learning. A debrief that never creates cognitive dissonance is a debrief that never changes anything.
A simple "What if" question can create cognitive dissonance in seconds — which is why it is the most powerful tool in the debrief toolkit.
⚠ Common Pitfalls — Mistakes Trainers Make in Debriefs
- Turning the debrief into a chat — warmth is good; lack of challenge is not
- Doing all the talking — if you are speaking more than 50% of the time, something is wrong
- Addressing every learning need in the session — you will run out of time and overwhelm the trainee
- Only reviewing the straightforward cases — the complex ones are where the real learning happens
- Forgetting telephone consultations — they carry the same clinical risk and educational opportunity
- Not debriefing home visits — these happen outside your eyeline and need explicit review
- Failing to document advised actions — this is the legal exposure mistake
- Easing off on ST3 too early — independent practice is earned, not assumed at the start of ST3
- Using the same format every time — mix up KSA, Bloom's, RCA, themed — keep it fresh
- Trainee is clearly thinking — you can see them working it out
- A moment of surprise — "Oh, I hadn't thought of that" — is a moment of learning
- The trainee leaves knowing one thing they will do differently next time
- The trainer leaves knowing something about the trainee they did not know before
- At least one teaching point has been linked to AKT or SCA relevance
- Any safety concerns have been documented in the patient record
- The trainee feels challenged but supported — stretched, not crushed
🧠 Memory Aid — The DEBRIEF Mnemonic
🟣 For Trainers — Teaching Pearls & Discussion Prompts
- Ask the trainee to identify their own learning needs before you offer yours — you will often be surprised at how insightful they are
- Track recurring themes across debriefs — if the same gap shows up three weeks in a row, this is a PDP (Personal Development Plan) item, not just a teaching moment
- Use the 13 Professional Capabilities as a mental checklist — which capability is this case best illustrating or testing?
- If the trainee seems overconfident, a well-chosen "What if" question is your most effective tool
- If the trainee seems demoralised, start with what they did well — specifically, not generically
- Consider recording one debrief per year (with the trainee's consent) and watching it back together — revelatory for both parties
- "Think back to the last patient you debriefed. What do you think their experience of the consultation was?"
- "What is the one clinical area that keeps coming up in your debriefs — and what are you going to do about it?"
- "If your trainer could see inside your head during that consultation, what do you think they would have found?"
- "Tell me about a case where you got it right. What made you get it right that time?"
- "If you were debriefing yourself, what would you say?"
💎 Real-World Wisdom — What Trainees and Trainers Actually Say
This section brings together recurring themes from GP trainee communities, UK deanery feedback, trainee forum discussions, and educator insights — the things people discover in real practice that rarely appear in the official handbooks. Everything here aligns with RCGP guidance and has been distilled into professional teaching points.
🙋 What Trainees Wish They Had Known Earlier
These are the insights that trainees consistently raise when reflecting on their early GP placements. Most are discovered the hard way — but they don't have to be.
Many trainees start out feeling like the debrief is a test they have to pass. They rehearse what they think the trainer wants to hear. The real shift comes when they realise it is a conversation — and that admitting uncertainty is actually the right answer. Trainers are not looking for perfection. They are looking for honest reflection and a willingness to grow.
Trainees consistently report that the most useful debriefs happen quickly — ideally the same day as the consultation. By the following week, the detail has faded. The emotional memory of a difficult case fades even faster. Aim to debrief while the case is still fresh. A brief, same-day debrief is worth far more than a long review days later.
The trainees who get the most from debriefs come with their own questions. "I was unsure about this blood result — can we look at it?" or "I didn't know how to handle when she started crying." Ownership of the learning agenda makes the debrief richer for both parties — and trainers consistently say it makes their job easier and more enjoyable.
A learning point you hear but don't write down is a learning point you will likely forget by tomorrow. Keep a simple notebook or a running notes document open during debriefs. Experienced trainees often use a simple two-column format: "what I learned" and "what I'll look up." This also feeds directly into FourteenFish ePortfolio learning log entries — turning a 10-minute debrief into documented reflective evidence.
One of the most common anxieties in early GP placements is feeling like you should already know what you don't know. You shouldn't. The debrief exists precisely because trainees are still learning. Saying "I wasn't sure what to do here" is not a failure — it is the start of the conversation. The trainers who describe the best debrief cultures say the same thing: the trainees who thrive are the ones who are honest about their gaps.
When a clinical question comes up in a debrief that neither the trainee nor the trainer can answer from memory, the best trainers open NICE CKS together and look it up. This models the behaviour GPs use in real practice — and it builds the habit of checking rather than guessing. Trainees who watch experienced GPs look things up stop feeling embarrassed about doing it themselves.
📊 The Debrief Quality Spectrum
Community experience consistently shows that debriefs fall across a spectrum — from ones that barely touch the surface to ones that genuinely change how a trainee practises. This diagram shows the difference.
🔧 Real-World Challenges — And How to Handle Them
These are the situations that trainers and trainees describe again and again when talking about debriefs. Each one has a practical solution.
This is one of the most commonly described challenges in trainer communities. The trainee gives one-word answers, won't speculate, and seems to shut down.
- Start with what they did well — specifically, not generically. "I noticed you checked for red flags in all three patients — that's good practice."
- Ask feelings first: "How did that consultation feel from your side?" This opens the door before clinical questions.
- Use hypothetical framing: "I'm not saying you did anything wrong — but if it happened again, what might you do differently?"
- Check the environment: is the debrief happening somewhere private and comfortable? Public spaces kill honesty.
The most commonly reported practical barrier to good debriefs across all training schemes is time pressure. An unprotected debrief is the first thing to get cancelled.
- Timetable it and protect it — a blocked slot labelled "debrief" in the rota is far harder to cancel than an informal agreement.
- Share the load: the debriefing GP does not have to be the trainer. Any qualified GP in the practice can debrief.
- A ten-minute focused debrief on two or three patients is far better than no debrief. Don't let perfect be the enemy of good.
- For near-independent ST3s: one brief check-in mid-session plus a 15-minute end-of-session review is often enough.
The trainee who thinks they already know everything is often the one most at risk of missing something important. Overconfidence in early ST3 is especially common.
- Use a well-chosen "What if" question to create cognitive dissonance quickly: "What if that patient had been 28 weeks pregnant — what would you have done differently?"
- Ask them to look up the answer in NICE CKS in real time — this often reveals the gap they didn't think was there.
- Pick a genuinely complex case from their list and go deep. Complexity is humbling for even the most confident trainees.
- Avoid confrontation — frame it as curiosity, not challenge: "I'm interested in how you reasoned through that one — walk me through it."
This happens far more often than it is discussed. A difficult consultation — a child who reminds them of their own family, a terminal diagnosis, an angry patient — can leave a trainee visibly shaken. Trainees frequently say this is the situation where the debrief mattered most.
- Address the emotion before the clinical content. "Before we go through the patients — how are you doing? There were some tricky ones today."
- Normalise the reaction: "Most GPs find that type of consultation hard. It doesn't mean you did anything wrong."
- Don't rush to fix it with teaching. Sometimes the trainee needs five minutes of acknowledgement before they are ready to learn.
- If distress is significant, the clinical learning can wait. Wellbeing comes first.
- Signpost to support if needed — the trainee's educational supervisor, VTS pastoral support, or GP Health Service.
When the same gap appears repeatedly across multiple debriefs — poor safety-netting, always missing the psychosocial story, prescribing errors — it is a signal that this needs more than a debrief conversation.
- Name the pattern explicitly: "I've noticed over the last few weeks that safety-netting is something we keep coming back to. Let's make this a formal learning need."
- Add it to the PDP (Personal Development Plan) in the FourteenFish ePortfolio — this creates accountability and a record of the development journey.
- Dedicate a tutorial session specifically to this topic — don't keep trying to address it in 5-minute debrief conversations.
- Consider whether this needs a joint surgery or a COT (Consultation Observation Tool) assessment to get a fuller picture.
International Medical Graduate (IMG) trainees often come from cultures where questioning or disagreeing with a senior clinician is seen as disrespectful. Debriefs can feel threatening in this context — even when the trainer has entirely good intentions.
- Explain the purpose and culture of UK debriefs explicitly at the start: "In this practice, we want you to tell us what you were thinking. There are no wrong answers — we want to understand your reasoning, not catch you out."
- Model disagreement yourself: "I might have done this differently, but I'd love to hear your thinking first."
- Explicitly reward honesty about uncertainty: "That's really good — admitting you weren't sure is exactly what safe practice looks like."
- Build the relationship before building the challenge. IMGs often need a few weeks to trust that the debrief space is genuinely safe before they open up.
- Remember that many IMGs were taught in a transmission model of education — they may never have experienced a Socratic, exploratory style of teaching. It may be genuinely new to them, not resistant.
💚 Debriefs and Trainee Wellbeing — The Overlooked Function
Most of what is written about debriefs focuses on clinical education and patient safety. But trainees and trainers who describe the best debrief cultures almost always mention something else: the debrief is also the safest place to talk about how you are actually feeling.
GP training involves emotional labour that most trainees were not fully prepared for. A well-run debrief creates the conditions for this to be acknowledged — not just the clinical decisions, but the experience of making them.
- Debriefing after difficult clinical events reduces the risk of moral injury and burnout in healthcare workers
- Trainees who feel psychologically safe in debriefs are more likely to disclose uncertainty and near-misses
- The act of verbalising a difficult consultation to a trusted listener is itself therapeutic — even before any advice is given
- IMGs in UK GP training particularly value debriefs that acknowledge the emotional difficulty of adjusting to a new healthcare system
- Start each debrief with a brief check-in: "How are you doing?" — not as a pleasantry, but as a genuine question
- Notice when a trainee seems flat, withdrawn, or more anxious than usual — address the person before the case list
- Normalise emotional reactions to difficult cases — they are a sign of empathy, not weakness
- Know when to signpost: GP Health Service (a free, confidential NHS service for doctors) exists precisely for moments when debrief support is not enough
📝 Using a Debrief Template — Simple Tools That Make a Big Difference
A recurring practical insight from both trainers and trainees is that having a simple, shared template dramatically improves the quality and consistency of debriefs. It keeps the conversation focused, ensures nothing important is missed, and creates a record that protects everyone.
| Patient (initials) | What the trainee did | What was discussed / advised | Action needed? |
|---|---|---|---|
| e.g. J.B., 45F | Started amoxicillin for URTI without checking if viral | Discussed delayed prescribing. Looked up NICE CKS together. | No action — plan was amended at time. Learning log entry advised. |
| e.g. M.R., 67M | Referred to cardiology but didn't arrange ECG first | Agreed ECG should be done before referral. Discussed referral criteria. | ACTION: DEBRIEF — arrange ECG before referral goes off |
The third column is the legal protection column — only needed when action is required. Most rows will have nothing in it. The ones that do matter enormously.
Dr David Hindmarsh, a UK GP, created a simple notes-and-tasks debrief template in clinical IT systems. The concept: for each patient discussed in a debrief, open the notes and either add nothing (if all is well) or add a brief task note prefixed "DEBRIEF —". This takes five seconds and creates a searchable, auditable record. It is the simplest legal protection available to any supervisor and requires no extra paperwork.
⭐ What Makes Trainees Rate a Debrief as Excellent
When trainees across UK deaneries describe the debriefs they found most valuable, certain themes come up again and again. This is their collective answer to: "What made it great?"
Psychological safety is the foundation. Without it, trainees perform rather than reflect.
Open, thoughtful questions — not leading ones — drive the deepest learning.
Trainees value being told explicitly why this matters — in practice and in the AKT/SCA.
Acknowledging how the consultation felt, not just what happened, makes trainees feel seen.
"I know exactly what I'm going to do differently" — the mark of a debrief that actually changed something.
The trainees who talk most in their debrief learn the most. Silence from the trainer is educational gold.
🎯 Trainee Guide — How to Get the Very Most From Your Debriefs
Your trainer brings the expertise. You bring the honesty. Together, that is a powerful combination. Here is how to play your part well.
🚦 Supervision Levels — The Traffic Light Model
This model is used across many UK deaneries to describe how supervision intensity should change as a trainee develops. It aligns directly with how debrief frequency and depth should shift over time.
ST1, new to GP
- Every consultation reviewed
- Supervisor available for every session
- Full debrief after every surgery
- 30-min appointment slots
- No independent decision-making
ST2/early ST3
- Selected patients reviewed
- Named supervisor per session
- End-of-session debrief, 30 mins
- 15-20 min appointments
- Growing independence — monitored
Late ST3
- Spot-check + random cases
- Named supervisor available
- 15-min end-of-session check-in
- 10-min appointments
- Approaching independence — review if concerns arise
Moving from red to amber to green is not a one-way journey. If clinical concerns emerge at any stage — a near-miss, a pattern of unsafe prescribing, an incident — the supervisor must return to closer supervision immediately. The traffic light system describes the current level of trust, not a status permanently achieved. Patient safety always overrides the presumption of growing independence.
🤫 What Nobody Tells You — The Hidden Curriculum of Debriefs
- The debrief is a relationship, not a procedure. The best debriefs happen between a trainee and a trainer who genuinely trust each other. That trust takes time to build — and it has to be earned by both sides. A trainer who listens well earns honest answers. A trainee who is honest earns a better debrief.
- The cases you don't bring up are often the most important ones. There is a natural tendency to present the neat cases and hide the messy ones. But the cases where you felt most uncomfortable are almost always the ones with the most to learn from. If you are tempted not to mention a case — that is usually a sign you should mention it first.
- Debriefs improve with repetition. The first few debriefs feel awkward for almost everyone — trainee and trainer alike. The pattern and rhythm develops over weeks. Don't judge the process by its first three sessions.
- Your trainer is not always right. This is rarely said, but it is true. Experienced GPs sometimes give advice that reflects personal practice rather than current evidence. If something does not sound right, check NICE CKS yourself. A good trainer will welcome this. A great trainer will model it.
- Debriefs are not just for when things go wrong. Some of the best debriefs happen when everything went well — and the trainer pushes the trainee to understand exactly why, so they can replicate it. "You managed that really well. Tell me what you were thinking at the point the patient became upset." That is the debrief that builds confidence that actually lasts.
- The quality of your debrief reflects the quality of your training practice. Not all training practices run debriefs the same way. If your debriefs feel perfunctory, rushed, or consistently one-directional, it is okay to raise this with your educational supervisor. You are entitled to high-quality supervision — it is part of your training contract.
The BMA/COGPED Guide to the Training Week (updated July 2024) confirms that debrief time must be included in every GP training session involving direct patient contact. As a guide, many deaneries include a 30-minute debrief slot per session. The precise ratio should be agreed between the trainee and supervisor based on training stage — but the entitlement to protected debrief time is explicit and contractual.
If your debriefs are being routinely cancelled or compressed, this is a legitimate concern to raise with your Training Programme Director. You are not being difficult — you are advocating for your training.
⚖ The Legal Tip — Protect Yourself as a Supervisor
Imagine a patient comes to harm after a trainee's consultation. You debriefed that day. You told the trainee what needed to be done. The trainee did not do it. The case goes to court. You have no record of what you advised. The trainee claims you never said it.
You are the supervisor. You will come under scrutiny.
The Simple Solution
Add a brief note to the patient record for any debriefed consultation where you identified an action that needed to be taken. This sounds like a lot of extra work — it is not.
If the trainee acted reasonably and safely — nothing to add. If something was missed or needs changing — add a short note. Those two lines protect you far more than any verbal reassurance ever could. Should anything go to court, the responsibility for failing to act will rest with the trainee who did not follow your documented advice — not with you.
AKT & Debriefs — 15 Ways Debriefs Prepare You for the AKT
The AKT tests applied clinical knowledge — and debriefs, done well, are one of the most efficient ways to build exactly that.
The AKT is 80% clinical medicine — and 80% of that clinical medicine comes from patients exactly like the ones you see in your surgery every day. Every debrief is an AKT revision session in disguise. The question is whether you use it like one.
- After every prescription reviewed — ask: "Is this first-line? What does NICE CKS say?"
- After every investigation ordered — ask: "What would you do with an abnormal result?"
- After every referral — ask: "What was the referral threshold? Was this a 2-week wait?"
- Any drug in the complex patient list — ask: "What monitoring does this drug need? How often?"
- At least once per month: a themed prescribing debrief for any ST3 approaching the AKT
SCA & Debriefs — 15 Ways Debriefs Prepare You for the SCA
The SCA tests how you consult — and you consult every day in training. Every debrief is a chance to refine exactly the skills the SCA examiners are looking for.
These phrases should be practised in real consultations until they feel natural. A debrief is the perfect place to ask: "Did you use something like this? How did it land?"
🏁 Final Take-Home Points
The Bottom Line — What Every Trainee and Trainer Should Walk Away Knowing
- Patient safety is the prime purpose. Educational value is real and important — but it never comes before confirming patients are not at risk.
- Debriefs are mandatory. They are not optional extras. Build them into the timetable and protect them.
- ST1 and ST2 every patient — no exceptions. They are not ready for independent practice. Review all of them, every session.
- Challenge beats chat. The most comfortable debrief is rarely the most educational one. Push. Ask "what if." Create cognitive dissonance.
- Document what you advise. A brief note in the patient record protects everyone — including you.
- Debriefs build AKT knowledge — if you use them that way. Ask about thresholds, first-line treatments, monitoring, and evidence. One lookup per debrief, consistently over months, builds an enormous knowledge base.
- Debriefs build SCA skills — if you use them that way. Ask about ICE, empathy, safety-netting, shared decision-making, and timing. The best SCA preparation is not a revision course — it is 18 months of well-debriefed real consultations.
- Use the DEBRIEF mnemonic. Danger first. Explore don't lecture. Bloom it. Reframe with "what if". Identify one or two learning needs. Exam relevance. Fix it in the record.
- The best debriefs leave the trainee thinking, not just reassured. If they are nodding and smiling throughout, you are probably not challenging them enough.
- Great debriefs change doctors. Slowly, patiently, case by case. That is the point of the whole exercise.
Bradford VTS — The Universal GP Training Website | Debriefs Page | Free educational resource for GP trainees, trainers, and TPDs | For educational use only — always verify clinical content against current guidelines