PDSA Cycles
Small steps, big changes — the improvement loop that actually works in the real world of general practice.
PDSA is the quality improvement engine behind almost every successful change in primary care. Whether you are running your first QIP or helping a trainee understand why small-scale testing beats grand plans, this page has everything you need — including the insights that trainees only discover after they have made the mistakes.
A hand-picked mix of official guidance and real-world GP training resources. Because sometimes the best pearls are not hiding in the official documents.
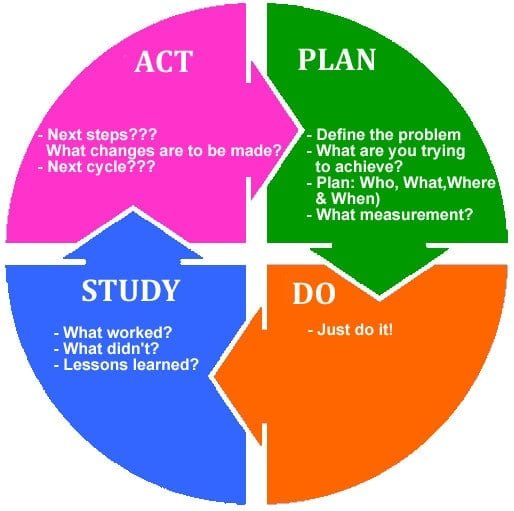
A 4-step loop: Plan → Do → Study → Act. Repeat until the improvement sticks.
Start small. Test on 5–10 cases first. Small is a feature, not a weakness.
Collect data before and after every change. No data = no evidence of improvement.
RCGP expects at least two PDSA cycles per QIP. Each one improves on the last.
Write up each cycle in real time. Reconstructing it later produces thin reflections.
The QIP section on FourteenFish. NOT the Learning Log. Assessors check the right section.
Before PDSA arrived, people tried two approaches to improvement — and both were deeply unsatisfying.
| Old Approach | The Problem | The Result |
|---|---|---|
| Trial and Error | No structure, no measurement, no plan | CHAOS — too much action, not enough thinking |
| Detailed Research Studies | Months of analysis, no change implemented | PARALYSIS — too much thinking, not enough action |
| PDSA Cycles ✓ | Structured, small-scale, iterative, measured | PROGRESS — real changes, evidence-based, manageable |
- GP practices are busy — small tests do not disrupt clinical care
- Each cycle builds knowledge before you commit to wider change
- It involves the whole team — receptionists, nurses, GPs — making change sustainable
- It mirrors the scientific method without needing a research budget
- The RCGP explicitly endorses it as the preferred QI methodology for GP training
- A failed cycle with good analysis is more valuable than a successful cycle with thin reflection
A PDSA cycle is a structured loop for testing a change, measuring its effect, and learning from the result. All four stages matter equally.
The PDSA Cycle — Four Stages
- Define the specific change you want to test
- Set your SMART aim
- Decide who does what, when, and how
- Make a prediction — what do you expect to happen?
- Agree how you will collect data to measure the effect
- Keep it small — 5 to 10 patients is fine for cycle one
- Carry out the planned change — just do it!
- Keep the scale small to reduce disruption and risk
- Record observations in real time
- Note unexpected events or problems as they happen
- Collect data as agreed in the Plan stage
- Analyse the data you collected
- Compare results with what you predicted
- Ask: did the change produce improvement?
- Identify what worked and what did not
- Look for unintended consequences or surprises
- Decide: Adopt, Adapt, or Abandon
- If adopting — consider wider rollout to the whole practice
- If adapting — design the next cycle with modifications
- If abandoning — try a completely different approach
- Document your decision clearly, with your reasoning
Sometimes a picture really is worth a thousand words. Here are visual representations of the key ideas in PDSA — designed to make things click instantly.
Every PDSA project begins by answering these three questions. They guide the whole process. Assessors love to see them clearly addressed in your write-up.
What are we trying to achieve?
Understand the problem clearly. Set a SMART aim: Specific, Measurable, Achievable, Relevant, Time-defined.
How will we know a change is an improvement?
Define your measures before you start. Collect baseline data. Without measurement, there is no evidence of improvement.
What changes might result in improvement?
What have others done? What do you think might help? What can you learn as you go? This is where PDSA cycles begin.
Here is the practical sequence for running a PDSA as part of your GP training QIP. Follow these in order and document each step as you go. Do not try to reconstruct the journey from memory at the end.
Spot a gap or problem in your practice
Look at consultation data, recent complaints, significant events, or things that simply "feel wrong." The best QIP topics come from genuine curiosity, not from trying to impress an assessor. Good examples: diabetic monitoring not being done, asthma inhalers not disposed of correctly, patients on warfarin missing INR checks, or B12 injections being given to patients who could safely switch to oral therapy.
Answer the three fundamental questions first
What are you trying to achieve? How will you know it is improved? What changes might help? Write these down before you do anything else. They become the backbone of your QIP write-up and every assessor wants to see them clearly answered.
Set a SMART aim
Example: "To increase the proportion of patients with Type 2 diabetes who have an HbA1c recorded in the past 12 months, from 60% to 85%, within 3 months." Specific. Measurable. Achievable. Relevant. Time-defined. This is what "above expectations" looks like to an assessor.
Collect baseline data before making any change
This is the most commonly missed step. Before doing anything, measure where you currently are. A simple search of 10–20 patient records is enough for cycle one. Without a baseline, you cannot show that your intervention made a difference.
Design PDSA Cycle 1 — small and specific
Choose one small change to test. Involve one member of the practice team. Run it for a defined period (a few weeks is fine). Document what you predict will happen, then what actually happens. 5 to 10 patients is the right scale for a first cycle.
Measure, reflect, and design Cycle 2
Study your results. Did the change work? Why or why not? What would you do differently? Design Cycle 2 based on what you learned from Cycle 1. The RCGP expects at least two cycles in a completed QIP.
Write a rich, honest reflection
Reflect on what you learned — not just what happened, but what you would do differently, what surprised you, and how this changes your future practice. Use the three-part framework: what worked well, what I would change, how this shapes my future. This is where most trainees leave easy marks on the table.
Upload to FourteenFish — in the right place
Complete the RCGP QIP template. Upload it to the dedicated QIP section of your FourteenFish ePortfolio. Not the Learning Log. Not the Audit section. The dedicated QIP section. Your Educational Supervisor then reviews and grades it before your ARCP.
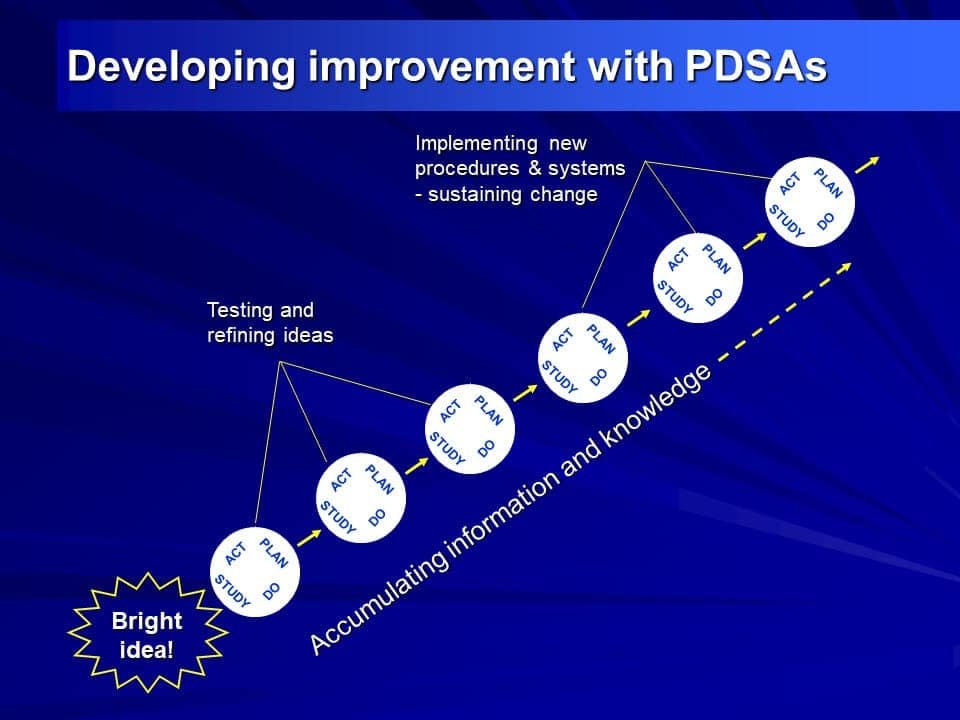
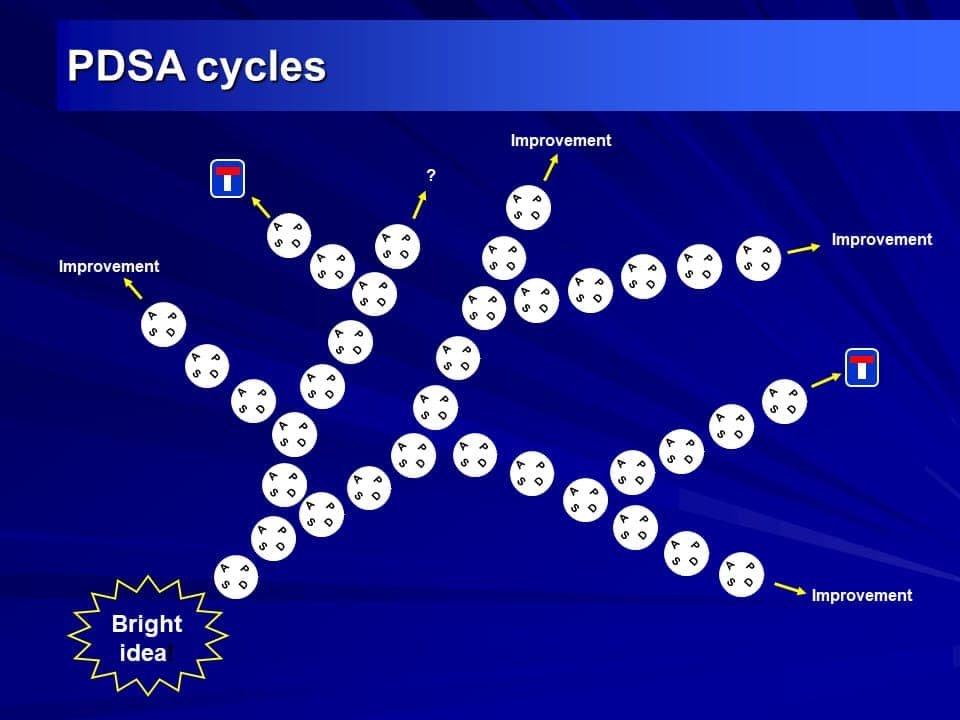
One PDSA cycle is just the beginning. The real power appears when cycles build on each other. This is why the RCGP requires at least two — and why trainees who run three or more consistently produce more impressive QIPs.
| Cycle | Purpose | Typical Scale | Key Question |
|---|---|---|---|
| Cycle 1 | Test the basic idea — does it work at all? | 5–10 patients or records | "Does this even help?" |
| Cycle 2 | Refine the approach based on what went wrong | 10–20 cases | "Does the improved version work?" |
| Cycle 3+ | Test the refined version; prepare for wider rollout | Larger; whole practice | "Is this ready to implement fully?" |
- Adopt — the change worked; implement it permanently across the practice
- Adapt — it partly worked; modify the approach and test again in cycle 2
- Abandon — it did not work at all; try a completely different approach
Assessors consistently comment that this explicit Adopt/Adapt/Abandon language signals mature QI thinking. Use it every time.
Here is how two PDSA cycles can build on each other to drive real, measurable improvement. This is the kind of project that receives strong marks at ARCP.
Gap identified: The practice notices that 40% of patients with Type 2 diabetes do not have an HbA1c result in the past 12 months.
SMART aim: To increase the proportion of diabetic patients with a current HbA1c from 60% to at least 80% within 3 months.
Baseline data: A search of 20 diabetic patient records finds that 8 out of 20 (40%) do not have a recent HbA1c. Well below the practice's 90% target.
- Practice Manager to identify 10 patients with overdue HbA1c by a set date
- Receptionists to phone patients and book a diabetic review with Dr Sans
- Dr Sans to explore barriers to monitoring (diet, medication, exercise)
- Prediction: most patients will attend if contacted directly
- Receptionists called all 10 patients
- 8 attended; 2 did not respond
- Data collected at each review appointment
- All 8 were apparently taking their medication
- 7 of the 8 were overweight
- 6 had a poor understanding of diabetes self-management
- 6 had never attended a Diabetic Structured Education Programme
- All 8 did little or no regular exercise
- Adapt — invited patients to a Diabetic Structured Education Programme
- Next cycle planned for 3 months later
- Result: HbA1c still poor; only 10% attended the programme
- Finding: the programme was too far away for most patients
- Contact the 8 patients to find out why they did not attend the external programme
- Ask whether an in-house session at the surgery would be more acceptable
- If yes — design a brief in-house education session before the nurse diabetic review
- All patients said the programme was too far away — they would come if it was at the surgery
- New in-house education room set up with short educational videos on diet and exercise
- Patients invited to watch a 15-minute video before their nurse review
- Nurse extended the discussion using basic motivational interviewing techniques
- Attendance rate at in-house education + diabetic review: 90%
- Patient satisfaction very high
- HbA1c improved to target range in 60% of patients after 3 months
- Adopted — in-house education model rolled out to all diabetic patients at annual review
- Team considered whether the model could work for other long-term conditions (asthma, COPD)
- Key reflection: the hidden barrier was distance, not motivation — something no guideline would have revealed
- The trainee did not give up when Cycle 1 failed — they used the failure to generate a better intervention
- The Study stage was rich — they found a hidden barrier (distance) that no official guideline mentions
- The ACT stage used explicit Adopt/Adapt/Abandon language with clear reasoning
- The reflection addressed the QI methodology itself, not just the clinical topic
Here is a clear summary of what the RCGP requires. Requirements can change — always verify with your Educational Supervisor and check the RCGP WPBA pages directly.
| Training Year | Requirement | Where It Goes on 14Fish |
|---|---|---|
| ST1 or ST2 (GP post) | 1 × QIP with at least 2 PDSA cycles | Dedicated QIP section — NOT the Learning Log |
| Years without a QIP | 1 × QIA per year | Learning Log entry on FourteenFish |
| End of training total | Minimum 1 QIP + 2 QIAs across all 3 years | Verified at ARCP |
- That the QIP is in the correct section of FourteenFish — not the Learning Log
- That your supervisor has assessed and graded it with every section complete
- That there are at least two documented PDSA cycles with data
- That the QIA is distinct from any LEA/SEA entries (which are a separate requirement)
- That you have a personal connection to the QIA — reviewing a national audit without personal data collection does not count
- That the write-up shows actual change was implemented, not just discussed
- 1. What are we trying to achieve? → Your SMART aim
- 2. How will we know a change is an improvement? → Your measurement plan
- 3. What changes might result in improvement? → Your PDSA intervention ideas
| Feature | PDSA Cycle | Clinical Audit |
|---|---|---|
| Purpose | Test and refine a change iteratively | Compare practice against an external standard |
| Scale | Small (5–20 cases per cycle) | Typically larger (whole practice or defined cohort) |
| Standard | Your own SMART aim | External standard (NICE guideline, QoF target) |
| Iteration | Built in — multiple cycles expected and encouraged | Re-audit is common but less formally iterative |
| Same thing? | Audit is one type of QI activity — not all QI is audit. Know the difference; your assessor will ask. | |
These patterns come up again and again in ARCP panel feedback and supervisor reviews. Read them once and avoid every single one.
| The Mistake | Why It Happens | What to Do Instead |
|---|---|---|
| Cycle 1 too large | Bigger feels more thorough | 5–10 patients for the first cycle. Small is the point. |
| No baseline data | Forgot to measure before starting the change | Collect baseline data first — always. Even 10 records counts. |
| Wrong 14Fish section | Assuming Learning Log = everywhere | QIP section, not the Learning Log. Check the section name before uploading. |
| Only one cycle | Running out of time in the post | Discuss timing with your ES at your very first meeting. Plan the timeline early. |
| Thin reflection | Treating reflection as a tick-box task | Write as you go. Use the three-part framework every time. |
| Supervisor not grading | Assuming it happens automatically | Chase your supervisor explicitly before your ARCP deadline. |
| LEA counted as QIA | Not knowing they are separate requirements | They are separate. You need both. Check your ARCP checklist. |
| No actual change implemented | Presenting data and recommendations without acting on them | The RCGP flags this explicitly: "discussion that change should happen" is not enough. You must actually implement it. |
Assessors consistently score higher when trainees reflect using all three of these:
- What worked well — and specifically why
- What I would do differently — with concrete reasons
- How this shapes my future practice — including QI methodology, not just the clinical topic
This three-part structure is explicitly referenced in the RCGP QIP feedback guidance. Use it every time you write a reflection.
These insights come from real patterns observed across UK GP training communities, deanery trainee forums, GP training support groups, and trainee peer accounts. Every single one has been verified against official RCGP and GMC guidance. None conflicts with it.
- Reference the three fundamental questions explicitly in your write-up
- Use a run chart (a simple line graph over time) rather than just a before/after table
- Name the team members who contributed and describe each person's role
- Use "Adopt / Adapt / Abandon" language at every ACT stage
- Explain what surprised you in the Study stage — surprises show genuine inquiry
- Address sustainability: what will still be happening in 12 months?
- Start your QIP in the first or second month of your GP post — timing matters
- Write one paragraph after each PDSA cycle immediately — you will thank yourself
- Pick a topic your trainer is already interested in — their enthusiasm is contagious and helpful
- Present your results at a practice meeting (even briefly) — it closes the loop and impresses assessors
- The FourteenFish upload timestamp is visible to assessors. Document as you go
- Starting Cycle 1 on all 200 diabetic patients — that is a full project, not a PDSA
- Having no baseline data ("we improved the template" is not enough)
- Uploading to the Learning Log instead of the QIP section
- Choosing a topic with no personal involvement in data collection
- Letting the supervisor grade go incomplete before ARCP
- Confusing audit and QI — they are related but not identical
- Rich curiosity about why something went differently than predicted
- A narrative of learning, not just a list of actions taken
- Evidence that the team was involved, not just informed
- A clear SMART aim that is genuinely SMART — not vague
- A three-part closing reflection: what worked, what I would change, how this shapes my future
If you are new to the UK NHS, some of the QI context may be unfamiliar. Here are a few things that help.
- QoF (Quality and Outcomes Framework) — a points-based incentive system where GP practices earn income for meeting clinical targets (e.g. percentage of diabetic patients with a current HbA1c). QoF data is often the source of your QIP baseline
- ARCP (Annual Review of Competence Progression) — your yearly portfolio review, similar to a progress committee in other systems. This is where your QIP is assessed
- FourteenFish (14Fish) — the UK GP training online portfolio where you document everything. It replaced the old RCGP ePortfolio in 2020
- PCN (Primary Care Network) — a group of neighbouring GP practices working together. Some QIPs span across a PCN rather than a single practice
- A great first step for IMGs: ask your trainer what your practice is currently working on for QoF — there may already be a natural QIP topic emerging from the data your practice is already reviewing
The best QIP topics share three features: they genuinely bother you, they matter to the practice team, and they are small enough to complete within your post. Topics involving whole-practice system overhauls are risky — you will spend months building consensus and run out of time before completing a second cycle.
Popular real-world topics from UK GP registrars that have scored well:
- Improving monitoring compliance for high-risk medications (lithium, methotrexate, DOACs)
- Reducing inhaler waste by improving disposal guidance at annual reviews
- Improving uptake of cervical smears in a specific patient group
- Improving documentation of safeguarding concerns in clinical notes
- Reducing same-day urgent appointment demand through better online triage signposting
- Improving frailty identification in patients over 75
- Ensuring B12-deficient patients on intramuscular injections are appropriately reviewed for oral therapy
These are all specific, measurable, and achievable within a 4–6 month post. That is not a coincidence.
The single most common reason a QIP stalls is not methodology — it is team engagement. Here is what actually works:
- Raise the topic at a practice meeting in your first month — do not surprise people weeks later
- Involve the receptionist or admin team from the very start. They hold the key to most QI interventions and they know the practice system better than anyone
- Never ask a busy member of staff to collect your data at short notice. Agree the plan together and allow them time to prepare
- Framing matters: "I would like your help improving this for patients" goes down much better than "I need to do a QIP for my portfolio"
- Present your results at a practice meeting. Even a brief five minutes closes the loop, respects the team's effort, and generates reflective evidence for your write-up
Many trainees feel anxious about the data side of a QIP. It does not need to be complicated:
- A simple before/after count on 10–20 patients is often sufficient for a first cycle
- Use the three types of measures: outcome (did HbA1c improve?), process (were patients actually invited?), and balancing (did any unintended harm occur?)
- Not all good QI needs numbers. A qualitative comparison of clinical notes before and after a documentation change is valid and acceptable
- Ask the practice manager or receptionist how to extract data from the practice system. They almost always know, and they will appreciate being asked
- A run chart (data plotted over time as a line graph) is far more compelling than a before/after table. It shows change dynamically. RCGP guidance explicitly recommends them. There is a free tool at the IHI website
- Discuss your QIP timeline at your very first Educational Supervision meeting
- Allow at least 8–12 weeks between Cycle 1 and Cycle 2 for the data to be meaningful. Two cycles completed within a fortnight are too short to demonstrate learning
- If you are an LTFT (less-than-full-time) trainee, allow proportionally longer. A 60% post gives you far less runway than a full-time six-month placement
- Never start a QIP in your final 6 weeks of a GP post. You will not complete a second cycle in time
- Ask your TPD whether your deanery runs a QIP peer group. Attend it. Trainees who use peer groups consistently produce better projects with less stress
The most powerful shift trainers report is moving trainees from seeing the QIP as a portfolio hoop to genuinely experiencing a small change they made actually improving care. The fastest way to create this shift is to share a brief personal story about a time your own practice's PDSA cycle revealed something that surprised you. Real stories from the room beat methodology lectures every time.
| Difficulty | Root Cause | Trainer Response |
|---|---|---|
| Cannot identify a topic | Looking for something "impressive" rather than something genuinely useful | Ask: "What has frustrated you clinically in the past month?" Start there |
| Makes Cycle 1 too large | Anxiety that small feels insufficient | Show them a real example of a small, high-quality first cycle. Small is the design principle |
| Thin reflection | Treats reflection as a form to complete rather than a conversation to have | Ask "What surprised you?" and "What would you tell a colleague starting this QIP?" — then have them write those answers down |
| Abandons QIP when Cycle 1 fails | Sees a failed cycle as a bad result | Reframe explicitly: a failed cycle with good analysis is more impressive than a successful one with thin reflection |
| Poor team engagement | Approaching QIP as a solo project | Ask them to name one receptionist and one nurse who are "on the team." If they cannot, the QIP has not really started yet |
- "What have you noticed at the practice recently that could be better for patients?"
- "How would you actually know if your change made a difference?"
- "If your first cycle shows no improvement — what are the three most likely reasons?"
- "Who in the practice is going to make this project succeed — apart from you?"
- "What will this practice still be doing differently in 12 months because of your QIP?"
- "Walk me through the Adopt/Adapt/Abandon decision — which did you choose and why?"
- "What does your run chart actually show? Does it tell a story?"
✅ Final Take-Home Points
- PDSA stands for Plan, Do, Study, Act — a structured loop for testing one small change at a time
- Always start with the three fundamental questions: they frame everything that follows
- Start small — 5 to 10 patients for the first cycle. Small is a feature, not a compromise
- Collect baseline data before making any change. Without it, you cannot prove improvement
- The RCGP requires at least two PDSA cycles in a completed QIP, and at least one QIA per year
- Upload the QIP to the dedicated QIP section of FourteenFish — not the Learning Log
- Document each cycle in real time. FourteenFish shows upload timestamps; reconstructing from memory is visible to assessors
- Failed cycles are valuable — a failed cycle with good analysis often scores better than a thin "success"
- Use Adopt/Adapt/Abandon language explicitly at each ACT stage and document your reasoning
- The best QIPs involve the whole team — the receptionist and practice nurse often hold the key to what actually works
- The write-up matters as much as the project itself. A brilliant project with a thin reflection is a missed opportunity