SCA STARTUP - PLAN & PREPARE
The biggest SCA resource on the web
- by Dr Ramesh Mehay
- Last modified: 11th January 2024
- No Comments
DOWNLOADS
WEBLINKS
……………………………………..
Information provided on this medical website is intended for educational purposes only and may contain errors or inaccuracies. We do not assume responsibility for any actions taken based on the information presented here. Users are strongly advised to consult reliable medical sources and healthcare professionals for accurate and personalised guidance – especially with protocols, guidelines and doses.
COME AND WORK WITH ME… If you’d like to contribute or enhance this resource, simply send an email to rameshmehay@googlemail.co.uk. We welcome collaboration to improve GP training on the UK’s leading website, Bradford VTS. If you’re interested in a more active role with bradfordvts.co.uk (and get your name published), please feel free to reach out. We love hearing from people who want to give.
……………………………………..
What is the SCA?
The RCGP’s SCA (Simulated Consultation Assessment) examination is basically a online remote set of patient consultations that are designed to challenge you in a number of areas – obviously the clinical (both your data gathering and management plans) and your interpersonal skills (i.e. how you interact and relate to others). The heart of the SCA examination lies in the use of patient simulators and skilled examiners. Patient simulators are advanced lifelike mannequins provide a safe and controlled environment for trainees to conduct physical examinations, make diagnoses, and prescribe treatments as they would with real patients. Your performance in this cases can then be evaluated without putting actual patients at risk.
How does it works on the day?
- 12 simulated consultations
- You have 12 minutes for each case
- Conducted remotely in a local GP surgery
- Can only be sat during ST3 training year
- Delivered across 9 months of the year – see full info on exam dates and booking windows
- You will have 3 minutes to read each case before it begins. Yes, there is 3 minutes between each case.
- You will have a rest period after 6 cases to allow for rest and mental rejuvenation.
- The exam can be both physically and mentally demanding. So, you must practice cases with your peers.

What is it testing?
You will be marked in 3 domains. These are
- Data Gathering which is your ability to take a good history AND understand the patient’s story, their concerns, and their expectations.
- Clinical Management – developing not just a good clinical management plan as per guidelines, but a SHARED plan where the patient is involved in the designing of that plan
- Relating to Others – which is basically the new term for INTERPERSONAL SKILLS. I prefer Interpersonal Skills to be honest as it is more clear and straightforward on what it is about. Basically, they are assessing your interpersonal and communication skills and how you use them to interact and relate to others (others being the patient, a relative, another health professional and so on). Yes, some of the cases might involve just the patient, the patient and a relative, the relative alone, or a concerned health professional like a District Nurse.
To do well in the above 3 areas, you need to be good at the following…
You will be tested on your medical knowledge and your ability to apply it in clinical scenarios. This includes their understanding of disease pathophysiology, diagnostic criteria, appropriate investigations, and evidence-based treatment options.
Important for Clinical Management.
The SCA exam assesses your communication skills, including your ability to establish rapport with patients, gather relevant medical histories, explore a patient’s or their relative’s ideas, concerns and expectations. It also includes providing clear explanations of diagnoses and treatment plans, developing shared medical management plans (rather than the doctor solely dictating it) and addressing the patient’s concerns effectively.
Important for Data Gathering & Relating to Others.
You will be evaluated on your ability to make sound clinical decisions based on the information available, prioritise patient care, and manage clinical scenarios efficiently and safely.
Important for Clinical Management.
The exam also considers your professionalism and ethical conduct, including their adherence to ethical principles, respect for patient autonomy, and maintaining patient confidentiality.
Important for Relating to Others.
You are expected to manage your time effectively during each simulated patient encounter, ensuring that you address the patient’s needs and concerns within the 12 minutes.
Important for all 3 areas – Data Gathering, Clinical Management & Relating to Others
The SCA examination often presents trainees with complex scenarios that require them to juggle multiple tasks, such as diagnosing a patient, managing their condition, and addressing patient communication simultaneously. Other times, it might be about managing 2 or more medical conditions (medical complexity).
Important for all 3 areas – Data Gathering, Clinical Management & Relating to Others
Trainees may encounter unexpected developments or complications during simulated patient encounters, and their ability to adapt and adjust their approach is also evaluated.
Important for all 3 areas – Data Gathering, Clinical Management & Relating to Others
Overall, the RCGP SCA examination is designed to provide a comprehensive assessment of your readiness to practice in the real-world setting of general practice. It tests not only your clinical knowledge but also your ability to handle the various challenges and complexities that arise in primary care settings while providing high-quality, patient-centered care.
Hang on... isn't clinical examination being tested?
No. Clinical examination is not being tested in this exam because this is hard to do remotely. For instance, how would you test for the anterior and posterior cruciates in a case that involved a knee injury? And the other great thing about this is that you do not need to bring any examination equipment (unlike the old CSA exam).
The RCGP say that Clinical Examination is tested in Work-Place Based Assessment – through your CEPs and the CSR comments on clinical examination.
How hard will the cases be?
The cases vary in complexity – some are very straightforward and others have different levels of difficulties – do not think that all of them are going to be very hard. This variety of cases is meant to reflect what happens in the real world and helps pick out those trainees who can handle a varying level of challenge. Those who can are deemed to be ready to become qualified GPs.
Will I be able to see the SCA examiner whilst I'm consulting with the SCA simulated patient?
No, you will not see the SCA examiner. Did you know that your cases are NOT actually marked in real time. Yes, you heard right – the examiner isn’t even there when you do the SCA exam – it’s just you and the patient. This is a good thing for you because it reduces something called the Hawthorne Effect – which is when your performance is not as good as it normally is just because you know someone is observing you which then puts you on edge, raises your anxiety levels and then makes you perform less well compared to what you usually do.
The examiners mark your cases several days after your live session. And a different examiner marks each case – it will NOT be the same examiner for all of the cases.
The examiners are not trying to fail you nor are they trying to trip you up...
Also remember that the SCA examiners are all GPs. They are not there to trip you up and they are definitely NOT trying to fail you. If anything, they want you to pass and they would be delighted to give you lots of marks – but they can only do that if you show that you are good enough. I’ve spoken to many trainees who have done the SCA and most of them say it is a really fair exam.
When should I do the SCA exam?
Well, you have to be in ST3. You cannot take it any earlier. SYou definitely need to have about 10-12 months experience and preparation time in a GP post. Therefore the best time to take it is probably at the beggining or middle of your ST3 post. Please make sure – when you book it, that you have enough GP training time to do another sitting should you fail. You don’t want to leave it right to the end of ST3, because if you fail, and have no GP training time left, you could be released from GP training!
In terms of practising for the CSA…
In the 1st month of a GP ST3 post
- Read up about SCA basics – what’s it testing, how it all works, visit the RCGP SCA pages and familiarise yourself with the SCA Bradford VTS pages.
2nd month
- Once you’ve settled into your GP post, gradually start practising some of the consultation micro-skills with real patients. A microskill is a small segment of a consultation skill – like exploring a patient’s ideas or explaining the diagnosis or management plant to them.
- Start reading a consultation book – this will help you identify consultation microskills you need to improve. (see section below on micro-skills)
Also start doing some COTs and look at these with your trainer. (more on this below too) - Start doing some Sit and Swap surgeries too (ask your GP trainer about these).
- With real surgeries, identify clinical areas you find difficult and brush up on these in a gentle way (e.g at the end of surgery or even in real time with patients if you can).
4-5 months BEFORE the exam
- 5-6 months before the exam – book it !
- Join or create an SCA study group. Trainees who are in SCA groups are more likely to pass as others will challenge and educate you. More on this below.
- Start practising SCA cases with others. Get those SCA(or old CSA) books and start meeting with others and practising at least on a weekly basis. Start doing some real heavy SCA work and practice. By the way, the cases in the old CSA books are mostly good and similar to what you will find in the SCA.
- At this stage, you may feel very pressured so remember to take regular breaks and to continue enjoying those nourishing activities in your life. If you find that you are not engaging with your former nourishing activities – you are going to burn yourself out. So make time for them because they will revitalise you and help you learn things in half the time.
Week before the CSA exam
- Calm down and take it easy. Let your brain breathe. Do not overload it. The more it can breath and feel relaxed, the better your performance will be in the SCA exam.
Diabetes at a Glance
SYMPTOMATIC
Symptoms of hyperglycaemia (polyuria /polydipsia, unexplained weight loss. visual blurring, genital thrush, lethargy) plus either:
HbA1c: 48mmol/mol or higher (LAB TESTING) (Type 2 diabetes is diagnosed in adults who are not pregnant and do not have haemoglobinopathy or haemolytic anaemia by a glycated haemoglobin (HbA1c) level of 48 mmol/mol or above.
The WHO state that diagnosis should be confirmed with a repeat HbA1c test, unless clinical symptoms and plasma glucose levels >11.1mmol/l are present in which case further testing is not required.)
FBG: >7.0mmol/L or higher x2
Dip urine to check for ketones
ASYMPTOMATIC
In the absence of symptoms – 2 abnormal results on separate days are required for the diagnosis.
Results:
- HbA1c > 48 mmol/l → repeat HbA1c test after 2 weeks → if HbA1c >48 mmol/l then code Diabetes and set recall
- HbA1c 42-47 mmol/l → code and set “at risk of diabetes” recall
May not be accurate in the following cases:
- ALL symptomatic children and young people
- Symptoms suggesting Type 1 diabetes/pancreatic insufficiency (any age)
- Short duration diabetes symptoms
- Patient at high risk of diabetes who are acutely ill
- Taking medication that may cause a rapid glucose rise e.g steroids, antipsychotics
- Acute pancreatic damage/pancreatic surgery
Patients with haemoglobinopathy – the labs test for this and will detect abnormalities.
A diagnosis of diabetes has important legal and medical implications for the patient and it is therefore essential to be secure in the diagnosis.
A diagnosis should never be made on the basis of glycosuria.
A stick reading of finger prick should be confirmed by a venous sample, as per NICE guidelines.
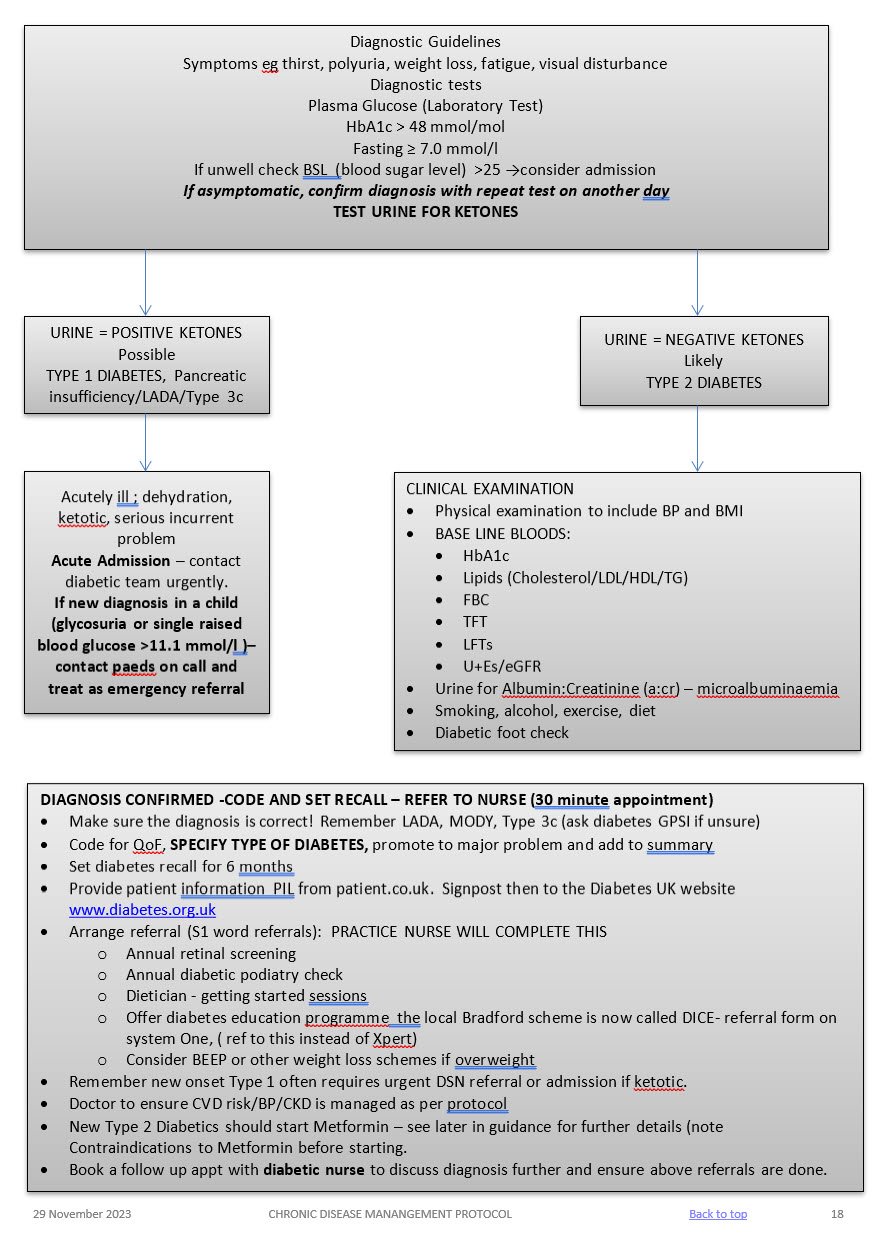
Admission
Admit to hospital if the person is at risk of a hyperglycaemic emergency (vomiting, abdominal pain reduced conscious level, heavy ketonuria, dehydration requiring IV fluids, hypotension, and serious intercurrent problem).
Same day referral
Refer to be seen on the same day if the patient is acutely ill, consider Type 1 Diabetes/pancreatic insufficiency if ketonuria present, the patient is slim and has a short history of marked symptoms (weight loss, thirst, and polyuria).
Early Referral
Diabetes and pregnancy requires referral to the hospital diabetes team
LIFESTYLE
BMI
Aim for healthy BMI <25 – consider dietition, Orlistat, other dietary measures & EXERCISE
ALCOHOL
Not to exceed recommended limits. (14 units men and women)
SMOKING
Stop!
BLOOD PRESSURE
Active management is essential!
Over half of all diabetics are hypertensive. Trials have shown that excellent BP control reduces retinopathy, nephropathy, strokes, heart failure and MI. BP control is as important as glycaemic control! TARGET < 130/80
Treatment
- 1st line – ACEi, ARB if they cannot tolerate it.
Ramipril starting regime derived from the HOPE study regime and BNF guidelines
If U&Es pre treatment reveal a creatinine < 150 micromol/l and a sodium >130 mmol/l then 2.5 mg Ramipril daily (1.25mg if on lower dose concomitant diuretics) for one week with check U&Es and an increase to 5.0 mg Ramipril for a further two weeks. Re-check U&Es and if indicated increase to 10mg Ramipril and repeat U&Es at least on an annual basis. If eGFR falls > 25% or creatinine rises by > 30% stop or back titrate treatment – see NICE guidelines. Don’t forget BNF cautions and contraindications. - 2nd line – CCB or, thiazide like diuretic or, Beta blocker (especially if there is a history of ischaemic heart disease),. Follow hypertension protocol
LIPIDS AND CVD RISK (see lipid modification protocol)
Offer generic Atorvastatin 40mg (Bradford Healthy Hearts) if their Q risk >10% (aged between 18-84 yrs), have been diabetic for > 10 years or, over 40 years old. Target chol <4mmol/l
For diabetics with established CVD offer secondary prevention or Chol > 4mmol/l – Atorvastatin 80mg
Triglycerides:
If TG level remains high (above 4.5mmol/l) please ref to CKS guidance on lipid modification or in-house lipid modification protocol.
Do not routinely offer Nicotinic acid or Omega fish oils.
MICROALBUMINURIA AND CKD
- All diabetics need testing annually for microalbuminuria and eGFR – microalbuminuria is the first sign of diabetic kidney disease and occurs before eGFR falls.
- SEE CKD PROTOCOL
ANTIPLATELETS
- Do not offer anti-platelets unless there is evidence of CVD
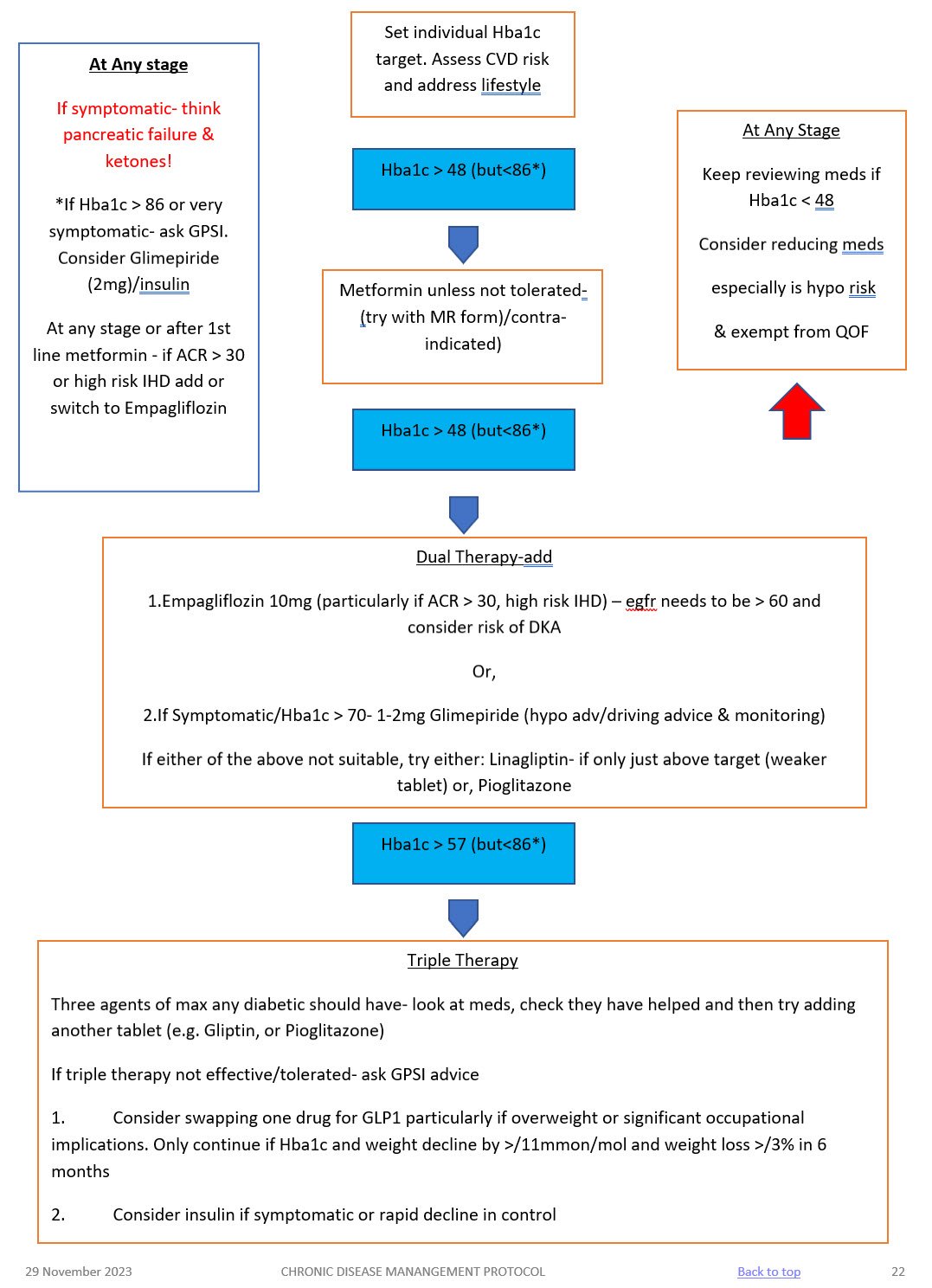
NICE recommended Hba1c targets are:
- 48mmol/mol – people who are managed by lifestyle and diet
- 48mmol/mol – people who are managed by lifestyle and diet combined with a single drug not associated with hypoglycaemia (such as metformin)
- 53mmol/mol – people who are taking a drug associated with hypoglycaemia (such as sulphonylurea), combination treatment
See table below for suggested targets for frail/elderly patients. Please exempt from QoF if you follow these targets putting an explanation in the notes.
Hba1c Target: aim for 48mmol/mol (if on diet or single drug not affected by hypoglycaemia ) or <53mmol/mol (if on SU, or more than one medication). Caution: elderly
- Start Oral treatment usually Metformin at diagnosis. Metformin 500mg ideally with evening meal, increasing to 1 gram a week later if they have no side effects.
- Please remember Metformin is very effective, reduces cardiovascular risk, retards weight gain and is not usually associated with hypos – but is contra-indicated if Creatinine > 150 (or eGFR < 40) in CCF or significant hepatic dysfunction.
- Metformin has to be stopped if eGFR fall below 30!
- Metformin MR can be used if they run into problems with GI side effects.
- Don’t forget that on starting hypoglycaemics to complete the prescription exemption form for those patients under 60 years of age.
- If you are starting a sulphonylurea (ideally Glimepiride) – ensure they are counselled and documented about:
- symptoms of hypos
- hypo management
- hypos and driving and remind them about informing their car and travel insurer AND document this in their records. If they hold HGV or PSV license then check with the 6 monthly updated DVLA guidance with respect to them having to inform the DVLA.
- Ensure they have been given a glucometer and a sharps bin, test strips and lancets are added to their repeat prescription
- DISCUSS AKI SICK DAY RULES ADVICE – see hypertension protocol for full advice.
FUNCTIONALLY DEPENDENT
- Due to loss of function, having impairments of ADLs
- Increased likelihood of requiring addition medical &/or social care
- HBA1c target: 53 – 64mmol/mol
FRAIL
– Combination of significant fatigue, recent weight loss, severe restriction in mobility & strength, increased propensity for falls & increased risk of institutionalisation
– A recognised condition & accounts for 25% of older people with diabetes
– Clinical Frailty scale or CHSA 9-point scale (assessment tool)
– HBA1c target: 60-70mmol/mol
DEMENTIA
– Degree of cognitive impairment leading to sig. Memory problems, a degree of disorientation, or a change in personality & unable to self care
– MiniCog tool (easy to use assessment tool)
– HbA1c target: 60-70mmol/mol
END OF LIFE CARE
- Significant illness or malignancy & have life expectancy reduced to <1 year
- Glycaemic aim – hypo and symptomatic hyperglycaemia avoidance
Medication | Mode of action | Side effects | Cautions (check BNF for more detail) | Dose |
METFORMIN 1st line treatment, unless BMI <25 (23 in South Asian population) Low Hypo risk Reduces CVD risk, weight neutral | Helps to stop the liver producing new glucose. It helps to overcome insulin resistance by making insulin carry glucose into muscle cells more effectively.
| Main side effect if GI affects, generally dose dependent-can be reduced with gradual increase in dose over several weeks or trying modified release Metformin Also: metallic taste, reduced absorption of vitamin B12, build up of lactic acid in the blood, allergic reaction and liver problems. | STOP/DO NOT USE IF eGFR <30 ml/min *Lactic acidosis- care if eGFR < 45ml/min. Document that advice has been given to stop these tablets if they become dehydrated (restart when eating normally again) *GI side effects. Titrate dose slowly to reduce side effects NOTE IF ALT> 3 TIMES NORMAL | Start at 500mg ideally with evening meal, increasing to 1g with evening meal after a week if they have no side effects. Max dose 2 gram over 4 weeks. Consider slow release for to reduce tablet load or if they are struggling with GI side effects.
|
SGLT-inhibitor Empagliflozin Low hypo risk Can help with weight loss | Sodium-glucose co-transporter 2 (SGLT2) inhibitor that prevents glucose reuptake in the kidney, leading to the excretion of excess glucose in the urine. | Polyuria, polydipsia, thrush. UTI, fluid depletion Increased risk of amputation- avoid if h/o leg ulcers | Only start if Cr Clearance > 60. Care if > 75 years. Risk of postural hypotension. Care needed if they have skin ulcers – risk of amputation. Document advice about normoglycaemic ketoacidosis and give ketostix. | Empagliflozin 10mg. Can be increased to 25mg. Expensive so only continue if there is a clear response after 6 months |
SULPHONYLUREA (SU) Glimepiride Risk of hypos Good if rapid response is needed. | They work by stimulating cells in the pancreas to make more insulin. They also help insulin to work more effectively in the body.
| Weight gain. Hypoglycaemia, gastrointestinal side effects, low sodium, facial flushing and intolerance of alcohol, allergies etc.
| Can cause hypoglycaemia, particularly if there is renal impairment or they are elderly. Consider occupation – hypos if not eating regularly, fasting. Make sure you give and document advice about hypos. Make sure they are able to test their blood glucose – issue glucometer, test strips, lancets and sharps bin. (SGBM) Document advice about driving/insurance. | Start at 1mg and titrate up to 4mg depending on glucose level. Should have an effect on Hba1c over a 2 month period. |
GLIPTIN Do not cause weight gain and encourages patient satiety. Although they probably reduce Hba1c levels less than other drug treatments. Low hypo risk | They work by blocking the action of the enzyme, DPP-4, which destroys the hormone Incretin.
| Gastro-intestinal effects, oedema, headache, Avoid if h/o Pancreatitis or heart failure or liver problems. | *Expensive- only continue if they meet NICE guidance. *Not v powerful max likely reduction ~ 11 mmol/mol *Do not use if a h/o pancreatitis *Monitor egfr at reviews *Don’t use if heart failure risk | Linagliptin 5mg if eGFR < 50 |
GLITAZONE Pioglitazone Low hypo risk Consider in people with very significant features of metabolic syndrome. South Asian | Reducing insulin resistance. Improving insulin sensitivity.
| Oedema esp if heart failure or at risk. Rare reports of liver dysfunction. Weight gain, gastro-intestinal side effects, headache, dizziness.
| Discuss with member of Level 2 team before starting. Avoid if they have heart failure or risk of fluid overload Avoid if h/o bladder cancer, undiagnosed haematuria Avoid if fracture risk Monitor LFTs at each diabetic review. Annual urine dip looking for haematuria | Pioglitazone:15mg-30mg. A six month period may be needed to really see an effect from these tablets. NICE recommends that they are only continued if at least a 11 mmol/l reduction in Hba1c is seen within 6 months of starting the treatment.
|
GLP-1 mimetic/insulin | Discuss with Level 2 doctor |
|
- At first warning of episode of hypoglycaemia:
- Immediately treat with a 15-20g of a short-acting carbohydrate such as:
- 200 mls of Lucozade (please note Lucozade formula has changed so lower in sugar- need 200ml)
- 200mls of non-diet drink
- 4-5 glucose tablets
- 3-4 jelly babies
- 200mls of fruit juice
- Immediately treat with a 15-20g of a short-acting carbohydrate such as:
- If the hypo is more severe, and the patient cannot treat themselves:
- applying Glucagel (or treacle, jam or honey) on the inside of cheeks and gently massaging the outside of cheeks.
- if unconscious, Glucagon can be injected if the person treating has been trained to use it.
- Otherwise call an ambulance immediately
- Important:
- If unable to swallow or unconscious, do not give anything by mouth (including Glucagel, treacle, jam or honey). Make sure family and friends are aware of this. If unconscious, place patient in the recovery position (on side with head tilted back) so that tongue does not block throat.
- Follow-on treatment:
- To prevent blood glucose levels dropping again, follow sugary foods with 10-20g of a longer-acting carbohydrate such as:
- half a sandwich
- fruit
- a small bowl of cereal
- biscuits and milk
- the next meal if due
- Patients experiencing regular episodes of hypoglycaemia require prompt review by the diabetes team.
- Severe episodes of hypoglycaemia require urgent review by the diabetes team.
- To prevent blood glucose levels dropping again, follow sugary foods with 10-20g of a longer-acting carbohydrate such as:
Advise patients the following: if you do go down with a cold, flu or any other illness…
- The Basics
- Rest.
- Drink plenty of sugar-free fluids.
- Avoid too much caffeine as this could make you dehydrated.
- Take painkillers in the recommended doses as necessary.
- Contact your GP to see if treatment with antibiotics is necessary.
- If you are vomiting uncontrollably, contact your GP or diabetes clinic.
- Insulin or diabetes medications
- Keep taking your insulin or diabetes medications even if you are not eating. Stop metformin and blood pressure medication if you are dehydrated. CONSIDER AKI SICK DAY RULES – see hypertension protocol.
- Testing
- Test your blood or urine four or more times a day and night (ie at least eight times in a 24-hour period) and write the results down. If you are not well enough to do this, ask someone to do it for you.
- Ketoacidosis
- When diabetes is out of control as a result of severe sickness, it can lead to a condition called diabetic ketoacidosis or diabetic coma if you have Type 1 diabetes. The body produces high levels of ketone bodies causing too much acidity in the blood.
- Testing for ketones
- If you have Type 1 diabetes and your blood glucose level is 15 mmol/l or more or you have two per cent or more glucose in your urine, you will also need to test your urine or blood for ketones. They are a sign that your diabetes is seriously out of control. Ketones are especially likely when you are vomiting and can very quickly make you feel even worse. If a ketone test is positive, contact your GP or diabetes care team immediately.
- Food and drink
- It is important to keep taking your medication as normal and drink plenty of sugar-free drinks. Aim to drink at least three litres (five pints) a day. Try to keep to your normal meal pattern, but if you are unable to, for any reason, you can replace some or all of your meals with snacks and/or drinks that contain carbohydrate such as yoghurt, milk and other milky drinks, fruit juice or sugary drinks such as Lucozade, ordinary cola or lemonade. You may find it useful to let fizzy drinks go flat to help keep them down
Advise patients of the following:
- Vaccinations and/or malaria tablets
- Carry diabetes ID or a GP letter if carrying insulin and list of prescription drugs
- Carry all medication and blood glucose testing equipment in hand luggage
- Consider how to keep insulin cool if travelling for long periods
- Travel insurance: – Allow 2 weeks to buy travel insurance. – Don‟t just buy on price, check the cover and read the small print – – Be honest and declare all medical conditions
- Plan to take twice the quantity of medical supplies normally used
- Consider adjusting medication if travelling across time zones
- Consider adjustment to insulin if travelling to hot or cold climate
- Carry a European Health Insurance Card (EHIC) if travelling within Europe
www.ehic.org.uk, / 0845 605 0707
Consider availability of insulin if travelling abroad for long periods.
Interpreting blood results on pathology template – Remember frailty
- HbA1c <48 →select satisfactory→take no action – patient will be reviewed as per recall
- HbA1c 48-53 →select abnormal →speak to nurse → send task to admin to book tel appt with nurse to discuss abnormal result and document a suggested plan to up-titrate medication based on the above guidance for nurse to discuss with patient – nurse will discuss with patient possible changes to medication and then task Dr back to make changes and issue script. – if on single drug or diet only
- HbA1c <53 → select satisfactory →take no action – if on SU or combination drugs patient will attend at next review 6 months later
- HbA1c >53 → select abnormal (take into account patients age and fraility) →speak to nurse → send task to admin to book tel appt with nurse to discuss abnormal result and document a suggested plan to up-titrate medication based on the above guidance for nurse to discuss with patient – nurse will discuss with patient possible changes to medication and then task Dr back to make changes and issue script.
Any concerns – send message to Level 2 team
Using the SystmOne Template (CDM) for Diabetes.
See CDM review table
- Bloods: U&Es, eGFR, HbA1c, ALT (if first year on statin) and lipid profile – (Consider other tests if have other chronic diseases.)
- Urine ACR.
- BP
- Lifestyle discussion: smoking status/cessation advice, exercise status, alcohol intake, diet.
- BMI
- Retinal review.
- Foot check annually (in house) and record on the template. If moderate or high risk they need a referral to podiatry
- Any complications? erectile dysfunction, neuropathic pain, autonomic neuropathy.
- Hypo unawareness, ? hypos requiring external intervention (see DVLA guidelines).
- Review of blood monitoring – if they require monitoring.
- Medication review: concordance/indications/side effects/if on insulin – injection sites.
- Record medication review done, move date on till next review
- Assign diagnosis to repeat template medication.
- Add/move recall on. NB: Diabetics well be reviewed at least 6 monthly.
TARGETS AT A GLANCE
- BP: <130/80 – particularly if there are renal problems
- Get to non smoking: don’t forget smoking cessation
- Cholesterol: < 4.0mmol/l
- HbA1c:
- Diet alone or single drug not affected by hypoglycaemia <48mmol/l
- Medication <53mmol/l. Patient tailored care needed especially if they are elderly or there are concerns about hypogylcaemia.
- BMI: <25
Diabetes in pregnancy is associated with risks to the woman and the developing fetus.
Planning a pregnancy
Women planning a pregnancy should be referred to a diabetes pre-conception clinic.
Pre-pregnancy planning includes:
- Diet and exercise, weight loss advised if body mass index > 27kg/m2
- Retinal photography unless carried out in last 12months
- Renal assessment (including microalbuminuria)
- Folic acid 5mgs for 3 months preconception and continued for first trimester.
- Establish rubella status, booster organised if required.
- Blood pressure should be monitored
- Smoking/alcohol cessation advice
Review of medications
- Metformin may be used before and during pregnancy, as well as or instead of insulin. The diabetes antenatal clinic will oversee their care whilst pregnant.
- Isophane insulin is the first-choice long-acting insulin during pregnancy.
- Discontinue oral hypoglycaemic agents (apart from metformin), ACE-inhibitors, Angiotensin Receptor Blockers and statins
Gestational diabetes
- 6 weeks post-partum patients require a HbA1c to establish whether glucose tolerance has returned to normal.
- All patients require advice on their elevated long term risk of diabetes.
- All patients require advice on their risk of gestational diabetes in future pregnancies.
- All patients require advice regarding diet, weight control and exercise
All patients require an ANNUAL HbA1c in view of their elevated risk of Type 2 diabetes. Please add an ‘AT RISK OF DIABETES’ recall to their notes.

What's it testing & how is it marked?
A lot of people think that the CSA is mainly testing consulting skills. And they believe that if you are a nice doctor, and that you are nice to the patient and give them all they want that the trainee will succeed and get through. THIS IS NOT TRUE. Yes, the CSA tests communication skills. But the CSA also pays equal importance to testing your history and examination skills (data gathering) and your clinical management of the case.
Here are the 3 domains being tested…..
DATA GATHERING
history, examination, consulting skills, ICE
Data gathering is where you do your history taking and examination. You will be tested on WHAT questions you ask (i.e. asking the right set of questions). In addition you will be tested on HOW you ask (communication skills) and whether you are methodical, structured and comprehensive.
CLINICAL Mx
diagnosis, NICE guidelines, share options, joint management plan.
Clinical management means synthesising what you’ve got from Data Gathering to form a reasonable working diagnosis. It also means that you know your guidelines (e.g. NICE), share options with patients, and develop a joint management plan with them. Of course, one needs to be mindful of co-morbidity and be flexible in their approach where clinically appropriate.
INTERPERSONAL SKILLS
consulting skills, rapport, respect, professionalism
Interpersonal skills is about you developing rapport with the patient. It also involves showing respect for them, for their point of view and being appreciative of the psycho-social impact of a disease on their life. You should show respect for others (like family members, other health professionals) and maintain a sense of professionalism. Interpersonal skills is more than just being a nice doctor!
You are basically given a mark for each domain. Each area has a maximum of 3 marks. That means each case has a total of 9 marks. There are 13 cases which gives a total of (13 x 9) = 117 marks. You generally need about 72-78 out of the 117 marks to pass – depends on how hard the cases are.
Click here to read more about each domain how the CSA is marked.
What sort of cases?
These are just a few examples. There are many!
- Breaking bad news
- Motivational interviewing
- Proxy consultations
- Confidentiality
- Lesbian, Gay, Bisexual & Transgender issues
- Aggressive patients
- Manipulative patients
- Negotiation Patients who request a test
- Patients who want antibiotics
- Non-compliant patients
- Somatising patients
- Joint pains
- Backache
- Dyspareunia
- Tired all the time
- Relationship break up
- Anxiety/panic attacks
- Non-specific chest pain
- Sexually Transmitted Infections
Prep 1 - start reading a consultation book
Although some people are naturally good at patient-centred consulting and others less so. But the good news is that these skills can be learnt. Yes! Even if you are not good at consulting in a person-centred way, with practice you can learn to be as good as those who are naturally good. Thats where a consultation book can help.
Of course, the key word here is practise! You can’t just read about the skills. You need to have a go at them and practise and play around with your words and phrases until you find ones that work for you. If you’re the type that likes to study – excellent! By all means do so. But please do not forget about PRACTISING. Without practice, you won’t acquire the SKILL. Would you be happy driving with a driver who said to you that he or she has never driven a car before but has read a book that teaches all the skills to do so?
Reading a consultation book or two will
- Help you get some of the cores communication skills to consult effectively with patients.
- Help you identify consultation micro-skills you need to work on and improve.
- Help you with your words and phrases.
- Help provide you with a consultation structure or framework.
Some good consultation books are…
- The Inner Consultation by Roger Neighbour (a great starter especially for ST1s especially if you like reading novels).
- Skills for Communicating with Patients by Silverman et al (one of the best core textbooks around – but can be a little heavy read).
- The Doctor’s Communication Handbook by Peter Tate (another great core text).
- The Naked Consultation by Liz Moulton (very much loved by GP trainees because it is easy to read and covers a variety of tricky scenarios).
Prep 2 - video yourself & start doing some COTs with your trainer

COT is short for Consultation Observation Tool. In other words – VIDEO WORK! Yes, videoing some of your patient consultations so that you can analyse your consultation style, communication skills and clinical approach with the patient. Many people feel apprehensive about showing themselves on video. This is a NORMAL REACTION – we all feel like that, even us educators!
But trust me when I say it is one of the most amazing ways of looking at yourself and seeing exactly where you can improve to become an even better doctor than you already are. Also trust me when I say that your trainer will be sensitive when reviewing your video with you. After a few sessions, you will no longer feel apprehensive about showing your consultation videos – in fact, you will want to! Reviewing your consultation videos will really help you pass the CSA. If you want to pass effortlessly, then pluck up the courage and overcome your fear and start doing some videos.
- And of course, don’t just video yourself for COTs. Video your real consultations for yourself and see how you talk and behave. You’ll notice things about you that you will want to change. You don’t always need a Trainer or TPD to advise you. You have it within yourself to reflect and advise yourself too.
- One last thing – if you’re in a CSA group – think about videoing the role-play interactions there too. Watch the video with other group members, yourself alone, and with your trainer or another qualified GP.
Why do I say video is key to CSA success? The thing is we often don’t realise we are doing certain things because we cannot watch ourselves. We don’t have a third eye. However, the video can be the thing you need to provide that third self-reflecting eye. See video as a window of CSA opportunity!
Prep 3 - Join or Make a CSA group
You have to get out there and practise – it’s the best way of achieving the level communication, clinical and interpersonal skills required to pass the CSA. The number of GP trainees I see that try to memorise stuff from CSA books is beyond belief – it’s crazy to rely heavily on books because what is being tested is not just what you know but what you say, how you say it and how you perform and interact with the patient. Good ‘performance’ can only be gained through regular practise, not through reading a CSA book!
Remember what I asked you earlier? Would you be happy driving with a driver who says that they’ve never really driven a car properly but they have memorised a book that teaches all driving skills?
Prep 4 - In the beginning... focus on the story, not the timer
You have 10 minutes per case in the CSA. But if you are just starting off, you should not worry about that. So, if you’re starting out on your CSA practice, forget having a timer (by the way, you should be start preparing for you CSA at least 6 months before the exam date). At this stage it is important that you focus on
- developing your consultation framework
- learning how to follow the story (the patient’s narrative)
- taking a good enough history and examination
- improving your explanations and
- learning how to formulate a joint management plan.
Later on, say 3 months before the exam, your consultation skills should be good enough. It is at this 3-month-before-the-CSA-date that you can start getting the timer out and trying to do it all in 10 minutes. And practice twice a week.
Prep 5 - Other things
Attend Mock CSA sessions
- All GP training schemes up and down the country run s either at HDR or externally.
- In fact, some Deaneries put on special mock CSAs throughout the year (like Yorkshire & the Humber do).
- Make sure you don’t miss out on these invaluable practise opportunities.
- Click here to go to the main CSA page on this website. We have loads of videos you can watch – videos on explanations, videos on whole CSA cases and more. Watch these.
- There are DVD resources you can buy too. Do a search on Amazon or something.
- Ask your trainer to do some role playing CSA sessions with you. Perhaps one half of the weekly tutorial can be devoted to this?
- Also ask them to look at your consultation videos not just via the COT proforma but via the CSA proforma too. Ask them to grade according to the three CSA domains: 1. Data Gathering 2. Clinical Management 3. Interpersonal Skills. Ask them to give you a score out of 3 for each one. 0=really bad. 1= fail. 2= pass. 3 = excellent
- During Sit and Swap surgeries (ask your trainer if you don’t know what these are) – ask your trainer if they can pick a couple of patients to asses CSA style.
- The biggest training session you have in your daily working life is normal surgery consultations with real patients.
- Many GP trainees will book weeks off to ‘study’ for the CSA – when actually, it’s the practise that is important. And what better way to practice your consultation and clinical skills than with real patients who present with a wide variety of things.
- If you get stuck with a patient – if it’s a clinical thing – look it up. If it’s a consultation skills thing – talk to your trainer.
- Reflect on
- your clinical knowledge
- you communication style and behaviour and the way you say things
- your attitude and behaviour
- This is a much better way of learning and improving your yourself than books – because it is all about how you perform at the end of the day rather than what is in your head! If you can’t get what’s in your head effectively out in the consultation then it isn’t really any good is it?
- The other great thing about seeing real patients in real surgeries is that the type of clinical things and the types of issues you will encounter will be similar to what pops up in the CSA exam. If you have seen lots and lots of real patients in real surgeries, then the cases that come up in the actual CSA exam should not surprise you. Equally, if you haven’t seen lots and lots of patients in real GP surgeries, the things that come up in CSA will not be familiar to you and you will struggle.
- Sit in with your GP trainer and observe him/her – this will open your eyes to alternative approaches, wordings and skills.
- Sit in with other health professionals, like the nurses, and observe how they do things like asthma reviews.
Final top tip – VIDEO YOURSELF
- VIDEO YOURSELF – not just for COTs.
- Video your own surgeries (with consent of course). And then watch them by yourself – you don’t always have to use a trainer or TPD. You’re an adult learner and you should be able to educate yourself.
- Video the role plays in your CSA study group – suggest it to them. You/They might not like it at first, but it is an incredibly powerful tool that can help you pass. By the end, you will love video work (or something closer towards love!).
- Like I said before, video provides that vital third external diagnostic eye that you can turn towards and reflect on yourself. It makes you aware of things you say and do which you would not be aware of otherwise. Sometimes what we think we have said or behaved is far from what actually was said or done. Video is the thing that will open your eyes. So video your surgeries and video your role plays in the CSA study groups. Watch some together with your trainer, TPD and trainees and watch some on your own.
Top Tips from Others
Please leave a comment below if you have any words of wisdom to help others or if you have any questions you wish to ask…